Warning: fopen(/home/virtual/enm-kes/journal/upload/ip_log/ip_log_2024-04.txt): failed to open stream: Permission denied in /home/virtual/lib/view_data.php on line 88
Warning: fwrite() expects parameter 1 to be resource, boolean given in /home/virtual/lib/view_data.php on line 89
Update from the 2022 World Health Organization Classification of Thyroid Tumors: A Standardized Diagnostic Approach
Thyroid Update from the 2022 World Health Organization Classification of Thyroid Tumors: A Standardized Diagnostic Approach
Keypoint The fifth edition of the World Health Organization (WHO) histologic classification of thyroid neoplasms released in 2022 includes newly recognized tumor types, subtypes, and a grading system. The classification of thyroid tumors has evolved based on classic histopathology and molecular pathogenesis. This review summarizes the major changes in the 2022 WHO classification of thyroid tumors and their clinical relevance.
1Department of Hospital Pathology, College of Medicine, The Catholic University of Korea, Seoul, Korea
2Cancer Research Institute, College of Medicine, The Catholic University of Korea, Seoul, Korea
3Department of Pathology, Kameda Medical Center, Kamogawa, Japan
4Department of Pathology, Cancer Genome Center and Thyroid Disease Center, Izumi City General Hospital, Izumi, Japan
Corresponding author: Chan Kwon Jung. Department of Hospital Pathology, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 222 Banpo-daero, Seocho-gu, Seoul 06591, Korea Tel: +82-2-2258-1622, Fax: +82-2-2258-1627, E-mail: ckjung@catholic.ac.kr
• Received: July 19, 2022 • Revised: August 24, 2022 • Accepted: August 29, 2022
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
The fifth edition of the World Health Organization (WHO) histologic classification of thyroid neoplasms released in 2022 includes newly recognized tumor types, subtypes, and a grading system. Follicular cell-derived neoplasms are categorized into three families (classes): benign tumors, low-risk neoplasms, and malignant neoplasms. The terms “follicular nodular disease” and “differentiated high-grade thyroid carcinoma” are introduced to account for multifocal hyperplastic/neoplastic lesions and differentiated thyroid carcinomas with high-grade features, respectively. The term “Hürthle cells” is replaced with “oncocytic cells.” Invasive encapsulated follicular and cribriform morular variants of papillary thyroid carcinoma (PTC) are now redefined as distinct tumor types, given their different genetic alterations and clinicopathologic characteristics from other PTC subtypes. The term “variant” to describe a subclass of tumor has been replaced with the term “subtype.” Instead, the term “variant” is reserved to describe genetic alterations. A histologic grading system based on the mitotic count, necrosis, and/or the Ki67 index is used to identify high-grade follicular-cell derived carcinomas and medullary thyroid carcinomas. The 2022 WHO classification introduces the following new categories: “salivary gland-type carcinomas of the thyroid” and “thyroid tumors of uncertain histogenesis.” This review summarizes the major changes in the 2022 WHO classification and their clinical relevance.
The World Health Organization (WHO) classification of tumors is updated regularly [1-4]. The fifth edition of the WHO Classification of Endocrine and Neuroendocrine Tumors was released as an online beta version (https://tumourclassification.iarc.who.int) in March 2022 [5]. Overview articles were published at the same time [2,6].
All volumes of WHO classification series organize tumors according to the anatomical site. In the fifth edition, each tumor is listed within a hierarchical taxonomic classification that is assigned based on the cell of origin, pathologic or molecular features, and biological behavior. The four main taxonomic ranks are category, family (class), type, and subtype. The majority of thyroid tumors are derived from follicular epithelial cells, while a small number arises from calcitonin-secreting C cells. Thymus, salivary gland, and germ cell tumors can present as primary thyroid neoplasms (Table 1). The fifth edition of the WHO classification includes newly recognized tumor types, subtypes, and a grading system. Follicular cell-derived neoplasms are categorized into benign tumors, low-risk neoplasms, and malignant neoplasms.
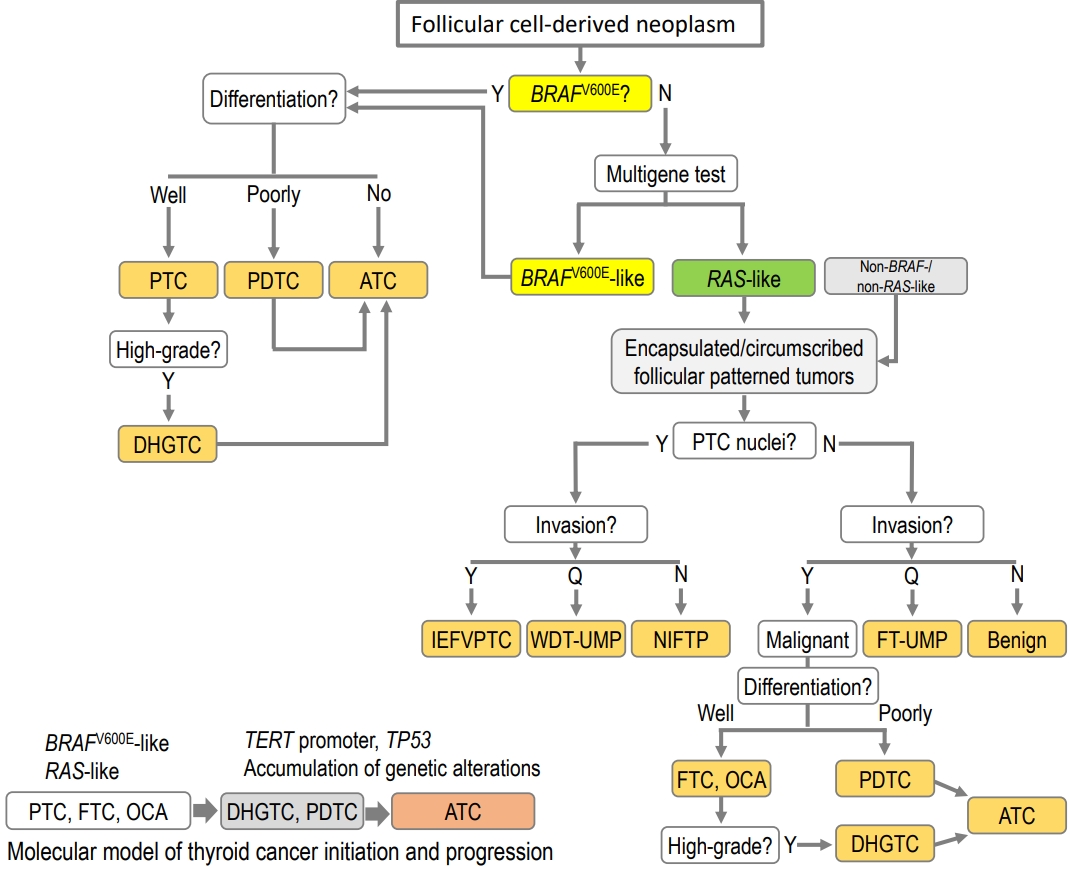
The classification of thyroid tumors has evolved based on classic histopathology and molecular pathogenesis. Most encapsulated/circumscribed thyroid tumors with a predominant follicular growth pattern exhibit a RAS-like molecular profile (Fig. 1) [7,8]. On the other hand, most thyroid tumors with a BRAFV600E-like molecular profile have papillary and/or infiltrative growth and florid nuclear atypia [7,8]. Both BRAFV600E-like and RAS-like thyroid cancers can gain additional genetic alterations and, as a result, progress to high-grade cancers [6].
Thyroid mesenchymal and stromal tumors, hematolymphoid tumors, germ cell tumors, and metastasis to the thyroid have been moved from the thyroid chapter to the respective standalone chapters in the same volume combining these entities from all endocrine organs.
This review aimed to provide a summary of updates in the 2022 WHO classification of thyroid tumors.
MAIN CHANGES IN THE 2022 WHO CLASSIFICATION
The main changes in the 2022 WHO classification compared against the previous edition are summarized in Table 2. The major revisions included modifications of the general terminology, the introduction of new entities, adoption of a grading system, and other changes specific to different tumor categories.
Changes in terminology
Historically, in thyroid pathology, the term “variant” has been used to describe the histologic subtype of a distinct tumor type, such as tall cell variant, columnar variant, hobnail variant of papillary thyroid carcinoma (PTC), clear cell variant of follicular thyroid carcinoma (FTC), papillary variant of medullary thyroid carcinoma (MTC), and so on. At the same time, “variant” is a commonly used genetic term, which means an alteration in the nucleotide sequence, and the genetic variant is increasingly being used in place of the term “mutation,” including for thyroid tumors. The new WHO classification uses “subtype” instead of “variant” in order to avoid confusion with genetic variants and to standardize the terminology across all the volumes of the fifth edition of the WHO classification. Therefore, the phrase “histologic variant” should be replaced with “histologic subtype.” When the term “variant” is used alone in the text of the WHO classification, readers should prioritize the genetic variant.
The term “Hürthle cell” is a historical misnomer [9]. In 1894, Karl Hürthle originally described the C cells of the thyroid gland as Hürthle cells in dogs. The new WHO classification has replaced “Hürthle cell” with “oncocytic cell.” As a result of this change, Hürthle cell adenoma and Hürthle cell carcinoma are now called oncocytic adenoma and oncocytic carcinoma (OCA), respectively.
For the designation of genes involved in gene fusions, the hyphen (-) or forward-slash (/) has been used as a separator between gene symbols, e.g., PAX8-PPARG (paired box 8-peroxisome proliferator-activated receptor gamma) or PAX8/PPARG. However, the separators should be replaced with a double colon (::) according to the HUGO Gene Nomenclature Committee recommendations [10], e.g., PAX8::PPARG.
New entities and reclassification
Before the fifth edition, the WHO classification of thyroid tumors included only neoplasms with morphology and behavior codes from the International Classification of Diseases for Oncology (ICD-O). Behavior codes of 0, 1, and 3 were assigned for benign tumors, borderline tumors (uncertain malignant potential), and malignancies, respectively. The 2022 WHO classification newly introduced tumor-like lesions for differential diagnosis purposes and convenience of the book readers (Table 1).
Developmental abnormalities include thyroglossal duct cyst, thyroid dysgenesis, and dyshormonogenetic goiter. The term “follicular nodular disease (FND)” was newly introduced to account for multifocal hyperplastic/neoplastic lesions occurring in the clinical setting of multinodular goiter. These lesions are not neoplastic and thus have no assigned ICD-O codes.
The new tumor type “high-grade follicular cell-derived carcinomas” has two histologic subtypes, traditional poorly differentiated thyroid carcinoma (PDTC) and a new subtype “differentiated high-grade thyroid carcinoma (DHGTC)” that arises from PTC, FTC, or OCA (Fig. 2). Another new diagnostic term is “thyroblastoma”; in particular, malignant teratoma or carcinosarcoma with Dicer 1, ribonuclease III (DICER1) mutation was renamed “thyroblastoma” (Table 1).
Invasive encapsulated follicular variant of papillary thyroid carcinoma (IEFVPTC) is now considered a separate entity and no longer a subtype of PTC (Table 1, Fig. 2). IEFVPTC has a RAS-like mutational and transcriptomic profile similar to that of FA and FTC (Fig. 1), whereas classic PTC and the infiltrative follicular subtype of PTC have BRAFV600E-like molecular profiles [11-15]. IEFVPTCs have a fibrous capsule or well-defined border and lack the histologic features of infiltrative follicular PTC. Like FTC, IEFVPTC can invade vessels in the capsule and develop distant metastasis.
In the fourth edition of the WHO classification, cribriformmorular thyroid carcinoma (CMTC) was classified as a distinct variant/subtype of PTC. However, it is no longer considered PTC and is now listed as a cancer type among thyroid tumors of uncertain histogenesis.
Adoption of a grading system and high-grade thyroid carcinomas
In differentiated follicular cell-derived carcinomas (PTC, FTC, and OCA) and MTC, high-grade histologic features include an increase in the mitotic activity and tumor necrosis (Fig. 2). Mitoses should be counted by expressing the number of mitoses per 2 mm2, which is roughly equivalent to 10 high-power fields (Fig. 3). The microscopic unit “high-power field” has been used for a long time. However, the high-power field is a non-standardized unit and should now be switched to square millimeters [16]. As the hotspot-counting method is recommended in thyroid pathology [17-19], the mitosis count should begin at the tumor region showing the highest mitotic activity.
DHGTC and PDTC are classified under the tumor type “follicular-derived carcinomas, high-grade” in the new 2022 WHO classification (Table 1). The new subtype DHGTC requires the presence of ≥5 mitoses per 2 mm2 and/or tumor necrosis (Table 3, Fig. 3). PTC, FTC, and OCA showing high-grade histologic features (mitotic count and tumor necrosis) are now classified as DHGTC (Fig. 2). The diagnostic criteria for PDTC have not changed. When an FTC has areas of solid or trabecular growth, it is important to examine the mitotic count and necrosis. When the mitotic count is ≥3 per 2 mm2 in solid or trabecular areas of the FTC, the tumor should be diagnosed as PDTC. When an FTC without solid or trabecular growth shows a mitotic count ≥ 5 per 2 mm2, the tumor should be diagnosed as DHGTC. Therefore, a prognostically relevant classification of thyroid carcinoma of follicular cells must take into account cellular differentiation and histologic grade (mitotic activity and/or necrosis).
The histologic grading scheme is newly applied to the diagnosis of high-grade MTC (Table 3). High-grade MTCs have at least one of the following three features: mitotic count ≥5 per 2 mm2, tumor necrosis, and/or Ki67 proliferation index ≥5% (Fig. 4). High-grade MTCs are associated with lower disease-specific survival and recurrence-free survival rates [19]. The Ki67 proliferative index is calculated as the percentage of positively stained tumor cells in a total of 500 to 2,000 tumor cells counted per tumor in hotspots [19]. Image analysis may assist in the accurate evaluation of the Ki67 index [18].
Changes in benign follicular lesions
Follicular cell-derived neoplasms are divided into benign tumors, low-risk neoplasms, and malignant neoplasms. Benign follicular cell-derived tumors in the new WHO classification include thyroid FND (although not all of these lesions are true neoplasms), follicular adenoma, follicular adenoma with papillary architecture, and oncocytic adenomas.
Multifocal benign nodules are clinically known as multinodular goiter and generally considered hyperplastic and non-clonal lesions. However, some lesions are molecularly clonal (i.e., neoplastic) and morphologically look similar to adenoma. Histologic criteria cannot always differentiate hyperplastic from neoplastic lesions. Therefore, a new term (FND) was introduced for these lesions. Follicular nodules in FND have the characteristic histologic findings of nodular hyperplasia. FND can have encapsulated cellular nodules that morphologically look similar to follicular adenoma, and thus, they cannot be differentiated based on histologic features. Given the variety of historical terms behind the group entity of FND, the WHO classification allows the use of the following synonyms: adenomatous nodule, adenomatous hyperplasia, nodular hyperplasia, and multinodular goiter.
Follicular adenoma with papillary architecture is generally an autonomous hyperfunctioning nodule and shows a characteristic intrafollicular papillary growth. In the previous edition of the WHO classification, this neoplasm was classified as hyperfunctioning adenoma (so-called toxic adenoma) within the category of follicular adenoma [1]. Follicular adenoma with papillary architecture and conventional follicular adenoma are different in that follicular adenomas with papillary architecture harbor mutations in the thyroid stimulating hormone receptor (TSHR), GNAS complex locus (GNAS), or enhancer of zeste 1 polycomb repressive complex 2 subunit (EZH1) genes while follicular adenomas usually harbor RAS mutations [20]. Among follicular adenomas that have a growth pattern of papillary hyperplasia, a tumor not associated with hyperfunction is called as follicular adenoma with papillary hyperplasia, which is classified within the follicular adenoma. It is important not to mistake these tumors for PTC. The papillae seen in follicular adenomas are broad edematous cores and lack PTC-type nuclei.
Changes in low-risk follicular cell-derived neoplasms
According to the new histopathological classification, low-risk neoplasms include non-invasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP), follicular tumor of uncertain malignant potential, well-differentiated tumor of uncertain malignant potential, and hyalinizing trabecular tumor. These neoplasms are regarded as borderline or uncertain behavior with ICD-O code of 1.
There were no changes in the diagnostic histologic criteria of these neoplasms. Although there was debate about the percentage (0% vs. <1%) of true papillae in the diagnostic criteria of NIFTP [21-24], the 2022 WHO classification maintained the original criterion (<1% papillae). If non-invasive follicular-patterned tumors fulfill the histologic criteria of NIFTP but have increased mitotic activity, the diagnosis differs depending on the mitotic count: <3 mitoses/2 mm2 does not change the diagnosis of NIFTP; 3 to 4 mitoses per 2 mm2 allow upgrading to encapsulated PTC with predominant follicular growth; and ≥5 mitoses per 2 mm2 qualified as non-invasive high-grade follicular variant of PTC that is DHGTC. Although diagnostic molecular tests are not mandatory (considered as “desirable diagnostic criteria”), the detection of BRAFV600E or telomerase reverse transcriptase (TERT) promoter mutations should exclude the diagnosis of NIFTP.
In the previous edition of the WHO classification, subcentimeter NIFTP and oncocytic NIFTP were not defined. However, tumors ≤1 cm in size and oncocytic tumors fulfilling the histologic criteria of NIFTP are now considered subtypes of NIFTP in the 2022 WHO classification [25,26]. The oncocytic subtype should be composed of 75% or more oncocytic tumor cells [25].
Encapsulated follicular-derived thyroid cancers
Encapsulated follicular-derived thyroid cancers include FTC, OCA, and IEFVPTC (Table 3, Fig. 3). For prognostic risk stratification of patients, all these tumors should be classified into minimally invasive (those with capsular invasion only), encapsulated angioinvasive, and widely invasive (those with entirely obliterated or focally intact tumor capsule and/or gross invasion through the gland) subtypes (Fig. 5). Encapsulated angioinvasive tumors are further divided into those with limited (<4 foci) or extensive (4 or more foci) vascular invasion. Extensive vascular invasion is often seen in widely invasive FTC, but extensive vascular invasion alone is not sufficient to diagnose widely invasive FTC.
Changes in papillary thyroid carcinoma
PTC subtypes include classic, encapsulated classic, infiltrative follicular, diffuse sclerosing, solid/trabecular, tall cell, columnar cell, hobnail, clear cell, spindle cell, Warthin-like, oncocytic, and PTC with fibromatosis/fasciitis-like/desmoid-type stroma.
In the fourth edition of the WHO classification, the follicular variants (subtypes) of PTC included infiltrative, encapsulated with invasion, macrofollicular, and diffuse or multinodular follicular subtypes. A noninvasive form of encapsulated follicular PTC does not exist in the WHO classification because of the introduction of NIFTP. Infiltrative follicular PTCs have florid nuclear atypia of PTC, stromal fibrosis, and psammoma bodies, and often show lymphatic invasion and lymph node metastasis. These histologic features are different from those of IEFVPTC (Fig. 6). In the 2022 WHO classification, there is no mention of the macrofollicular and multinodular follicular subtypes.
Among PTC subtypes, aggressive histologic subtypes include tall cell, columnar cell, and hobnail PTCs. The aggressive PTCs usually occur at an older age, are often associated with angiovascular invasion and advanced pathologic stage, and show increased mitotic activity. However, such aggressive PTCs with an indolent clinical course occur at a young age, are usually encapsulated or well circumscribed, and show a low mitotic activity and low Ki67 labeling index [27-31].
In the previous WHO classification, papillary thyroid microcarcinoma was a distinct subtype/variant of PTC. However, in the 2022 WHO classification, it is no longer considered a subtype because the microcarcinoma implies any histologic subtype of PTCs measuring ≤1 cm. Aggressive subtypes can occur as microcarcinoma. Therefore, subcentimeter PTCs require further histologic subtyping according to their histologic characteristics, such as classic papillary microcarcinoma, tall cell papillary microcarcinoma, and so on. The 2022 WHO classification reworded the term “encapsulated variant” into “encapsulated classic subtype” of PTC.
The criteria of tall cell PTC have been redefined. In the previous edition, tall cells were defined as cells that are two to three times as tall as they are wide. However, the newly adopted diagnostic criteria require that tall cells must have a height of at least three timestheir width and show dense eosinophilic cytoplasm and distinct cell membranes (Fig. 7A, B). The tall cell subtype should be composed of at least 30% of tumor cells qualified as tall. In a Japanese study, disease-free survival was shorter for tall cell PTC patients with a high Ki67 labeling index (≥5%) than in those with a lower Ki67 labeling index [27].
Hobnail PTC shows a mixed papillary and micropapillary structure and dyscohesive tumor cells. Hobnail cells have more pronounced nuclear atypia than those seen in classic PTC (Fig. 7C, D). It is important for pathologists to recognize the histologic findings mimicking features of hobnail PTC. The histologic mimic “hobnail-like morphology” can be found in more than 30% of classic PTCs [28]. Encapsulated or well-circumscribed classic PTCs often show cystic changes and have edematous and hyalinized papillae lined by hobnailing tumor cells (Fig. 7E, F). The hobnail-like morphology is considered degenerative atypia and not a true hobnail subtype. Patients with PTC showing hobnail-like morphology are younger and have a lower rate of aggressive clinicopathologic features and a better prognosis than those with hobnail PTC [28]. Therefore, a diagnosis of hobnail PTC in the absence of aggressive clinical and pathologic features (high mitotic count, prominent extrathyroidal extension, etc.) should be rendered with confidence only after excluding low-risk PTC.
The tumor previously known as the “cribriform-morular variant of PTC” is no longer a PTC subtype. A new term, CMTC, is now listed among the tumors of uncertain histogenesis.
Changes in anaplastic thyroid carcinoma
Anaplastic thyroid carcinoma (ATC) may show variety of histologic patterns, including epithelioid cell, spindle cell, giant cell, pleomorphic cell, small cell, squamous cell, rhabdoid, angiomatoid, or paucicellular; however, the WHO classification has not defined subtypes of ATC based on the predominant pattern.
Primary squamous cell carcinoma of the thyroid, listed separately in the previous edition of the WHO tumor classification, is now considered a histologic pattern of ATC. ATC with the squamous cell carcinoma pattern has more frequent BRAFV600E mutation rate and PAX8 immunopositivity than other ATCs [32,33]. Squamous differentiation can be seen not only in ATC, but also in other types of thyroid tumors, including PTC, FTC, PDTC, MTC, mucoepidermoid carcinoma, and intrathyroidal thymic carcinoma [34]. In particular, the histopathologic features of intrathyroidal thymic carcinoma may mimic those of ATC with the squamous cell carcinoma pattern or metastatic squamous cell carcinoma. These tumors must be differentiated from intrathyroidal thymic carcinoma because the latter has better clinical outcomes, with a 10-year survival rate of more than 80% [35].
Thyroid carcinomas of salivary gland-type and uncertain histogenesis
One important change in the 2022 WHO classification is the addition of a new category, thyroid tumors of uncertain histogenesis, including sclerosing mucoepidermoid carcinoma with eosinophilia (SMECE) and CMTC. In the 2017 WHO classification, SMECE was considered a subtype of salivary gland-type carcinomas of the thyroid gland.
A category “salivary gland-type carcinomas of the thyroid” in the 2022 WHO classification includes mucoepidermoid carcinoma and secretory carcinoma previously known as mammary analogue secretory carcinoma.
Fusion genes are hallmarks of salivary gland-type carcinomas of the thyroid. Secretory carcinoma and mucoepidermoid carcinoma are characterized by specific fusion genes (ETV6:: NTRK3 [ETS variant transcription factor 6::neurotrophic receptor tyrosine kinase 3] and CRTC1 [CREB regulated transcription coactivator 1] or CRTC3::MAML2 [CREB regulated transcription coactivator 3::mastermind like transcriptional coactivator 2], respectively) [36,37]. However, these gene fusions are typically not found in SMECE [38-40]. SMECE is morphologically different from mucoepidermoid carcinoma of the thyroid, although epidermoid and mucous cells are observed in both tumor types. SMECE is always associated with chronic lymphocytic thyroiditis showing a marked sclerotic background and infiltration of lymphocytes and eosinophils. The lack of common mutations found in differentiated thyroid tumors (BRAFV600E, RAS, and other mutations or gene fusions) further supports the proposal that SMECE is distinct in origin from salivary glandtype carcinoma and follicular cell or C cell-derived carcinomas [38]. Both solid cell nests and SMECE share immunophenotypic characteristics (p63-positive and thyroglobulin-negative) as shown in Table 4. SMECEs are therefore presumed to arise from solid cell nests (ultimobranchial body remnants) [38,40-42]. Genetic alterations found in some cases of SMECE include MET hyperploidy and mutations in the APC regulator of WNT signaling pathway (APC), neurotrophic receptor tyrosine kinase 3 (NTRK3), and neurofibromin 1 (NF1) genes [38,40,43].
CMTC was classified as a distinct subtype of PTC in the previous WHO classification because its papillary pattern and nuclear features are similar to those of classic PTC. However, CMTC has a different molecular profile from that of PTC. CMTC has genetic alterations involved in the Wnt/beta-catenin pathway, such as mutations in the APC and CTNNB1 (catenin beta 1) genes [44,45]. There have been no cases of CMTC with BRAFV600E. In terms of immunohistochemistry, tumor cells show nuclear expression of beta-catenin and express estrogen receptor and progesterone receptor [44,46,47]. These tumors have no colloid formation and are often negative for markers of thyroid follicular cell differentiation, such as thyroglobulin and PAX8 [45]. The cribriform component shows thyroid transcription factor 1 (TTF1) positivity, but morulae are negative.
Other tumors
Changes pertinent to PDTC and MTC have been described in the section “adoption of a grading system and high-grade thyroid carcinomas” above. Thymic tumors arising within the thyroid gland include thymoma, intrathyroid thymic carcinoma, and spindle epithelial tumor with thymus-like elements (SETTLE). There are no changes in the diagnostic criteria of these tumors. Thyroblastoma is an exceptionally rare embryonal high-grade thyroid neoplasm composed of primitive follicular cells, small cells, and mesenchymal stroma. The most common genetic alterations found in thyroblastoma are somatic DICER1 mutations [48,49]. Thyroblastoma is a new term for malignant teratoma and carcinosarcoma associated with DICER1 mutations in the thyroid gland [48-50].
REMARKS FOR CLINICIANS
For clinicians, the most important change in the 2022 WHO classification is the introduction of the two-tiered grading system, allowing the distinction of high-grade cancers from well-differentiated follicular cell-derived carcinomas and MTC. DHGTCs exhibit more advanced histopathologic stages and lower radioactive iodine avidity than well-differentiated thyroid cancers (PTC, FTC, and OCA) [51-53]. The overall prognosis of DHGTC is similar to that of PDTC [52]. High-grade MTCs occur in approximately 25% of cases and have worse prognosis than low-grade MTC [19]. Therefore, patients with DHGTC and high-grade MTC require more intense treatments and should be more closely followed up for recurrence.
Clinicians and pathologists need to be aware of new terminologies and classification schemes. The updated WHO classification and nomenclature will have a further impact on the upcoming releases of clinical guidelines, cancer staging protocols, thyroid histopathology reporting standards, and cytology reporting systems.
CONCLUSIONS
Recent advances in the molecular pathogenesis of thyroid tumors have improved our understanding of tumor origin and evolution and impacted their diagnostic criteria. Thyroid tumors are now classified based on the tumor cell of origin and molecular profile. The concept of low-risk neoplasm and histologybased grading systems help guide personalized therapeutic decisions for patients at different levels of risk. These changes are continuing, and new updates in the WHO classification of endocrine neoplasms are expected in the next 5 years.
Article information
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This research was supported by a grant (NRF-2020R1F1A1070028) from the Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Science and ICT. This research was also supported by a grant (HI21C0940) from the Korean Health Technology R&D Project, Ministry of Health &Welfare, Republic of Korea.
Fig. 1.
Molecular classification and histopathological correlates in follicular cell-derived neoplasms. Thyroid neoplasms are classified as two molecular groups (BRAFV600E-like and RAS-like) or three groups (BRAFV600E-like, RAS-like, and non-BRAFV600E-/non-RAS-like) based on the mutational and gene expression profiles [7,8]. The BRAFV600E group is most commonly represented by papillary thyroid carcinoma (PTC). The BRAFV600E-like molecular profile includes the BRAFV600E mutation and gene fusions involving BRAF, RET, and neurotrophic receptor tyrosine kinase 1/3 (NTRK1/3). RAS-like molecular profiles include NRAS, HRAS, KRAS, EIF1AX, enhancer of zeste 1 polycomb repressive complex 2 subunit (EZH1), Dicer 1, ribonuclease III (DICER1), phosphatase and tensin homolog (PTEN) mutations, BRAFK601E, and gene fusions involving peroxisome proliferator-activated receptor gamma (PPARG) and THADA. When the three-group molecular classification is applied, PAX8::PPARG gene fusion and mutations of EIF1AX, EZH1, IDH1, SOS1, SPOP, DICER1, and PTEN genes are classified as a non-BRAFV600E-/non-RAS-like group [8]. Encapsulated/circumscribed thyroid tumors with a predominant follicular growth pattern generally have a RAS-like molecular profile. High grade is histologically defined as the presence of ≥5 mitoses per 2 mm2 and/or tumor necrosis. Y, yes; N, no; Q, questionable; PDTC, poorly differentiated thyroid carcinoma; ATC, anaplastic thyroid carcinoma; DHGTC, differentiated high-grade thyroid carcinoma; IEFVPTC, invasive encapsulated follicular variant of papillary thyroid carcinoma; WDT-UMP, well-differentiated tumor of uncertain malignant potential; NIFTP, non-invasive follicular thyroid neoplasm with papillary-like nuclear features; FT-UMP, follicular tumor of uncertain malignant potential; FTC, follicular thyroid carcinoma; OCA, oncocytic carcinoma of the thyroid; TERT, telomerase reverse transcriptase; TP53, tumor protein p53; PAX8, paired box 8.
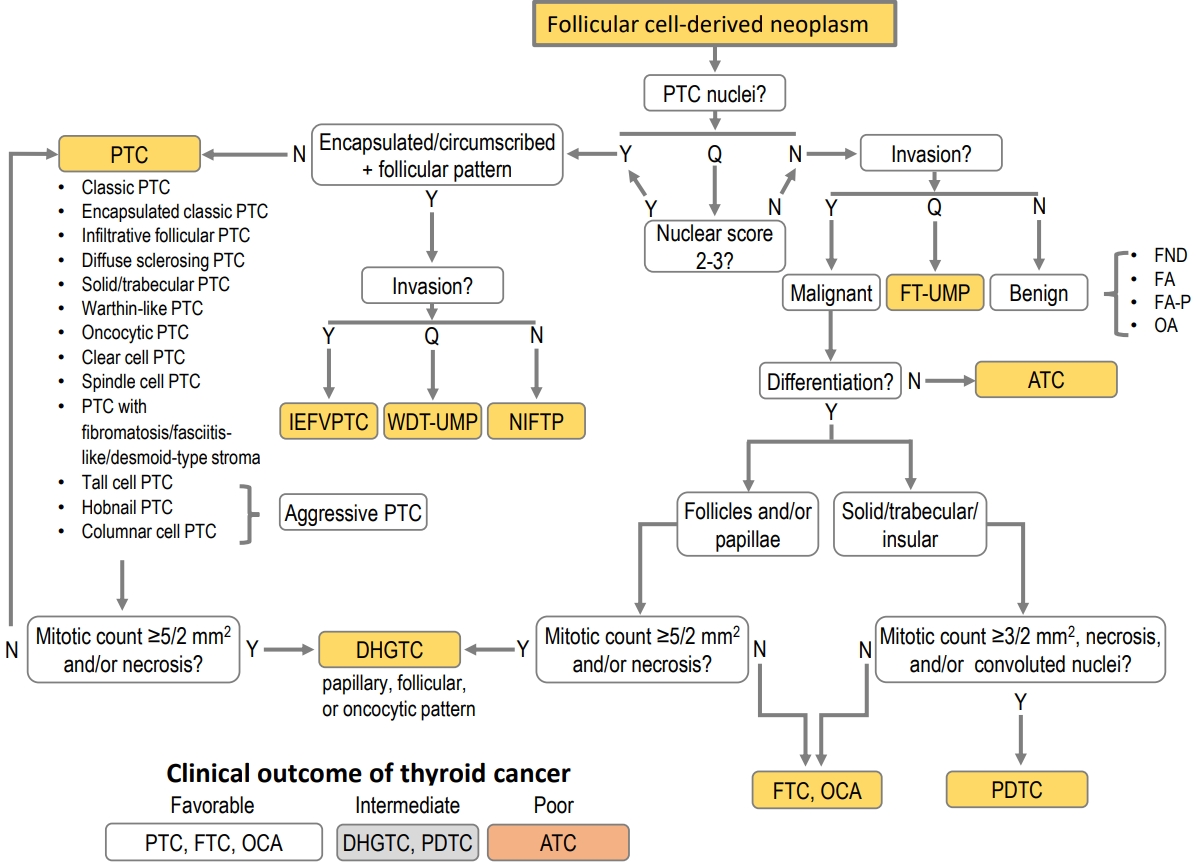
Fig. 2.
Decision tree for the differential diagnosis of follicular cell-derived neoplasms. The first step is to evaluate whether the tumor has nuclear features of papillary thyroid carcinoma (PTC). Tumors are then stratified according to the growth pattern, histologic differentiation, tumor capsular or vascular invasion, and high-grade histologic features. Y, yes; N, no; Q, questionable; FND, follicular nodular disease; FA, follicular adenoma; FA-P, follicular adenoma with papillary architecture; OA, oncocytic adenoma; FT-UMP, follicular tumor of uncertain malignant potential; IEFVPTC, invasive encapsulated follicular variant of papillary thyroid carcinoma; WDT-UMP, well-differentiated tumor of uncertain malignant potential; NIFTP, non-invasive follicular thyroid neoplasm with papillary-like nuclear features; FTC, follicular thyroid carcinoma; OCA, oncocytic carcinoma of the thyroid; DHGTC, differentiated high-grade thyroid carcinoma; PDTC, poorly differentiated thyroid carcinoma; ATC, anaplastic thyroid carcinoma.
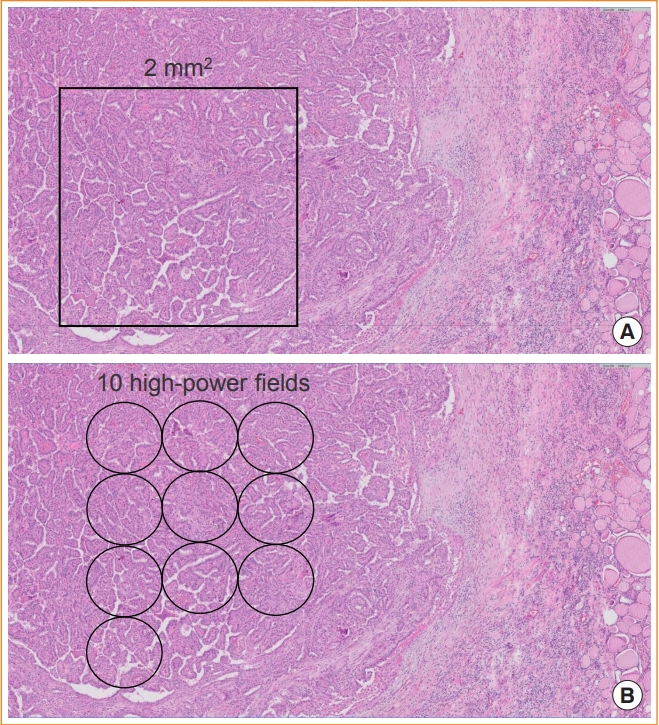
Fig. 3.
Counting mitoses in a hotspot. (A) The mitotic count is assessed by counting the number of tumor cells with mitosis per 2 mm2 in a hotspot (hematoxylin and eosin [H&E] stain, digital zoom ×10). (B) One high power-field of ×400 magnification using the ×40 objective lens and ×10 eyepiece has a field diameter of 0.49 to 0.53 mm in usual light microscopes (H&E stain, digital zoom ×10). Ten fields are approximately equivalent to 2 mm2.
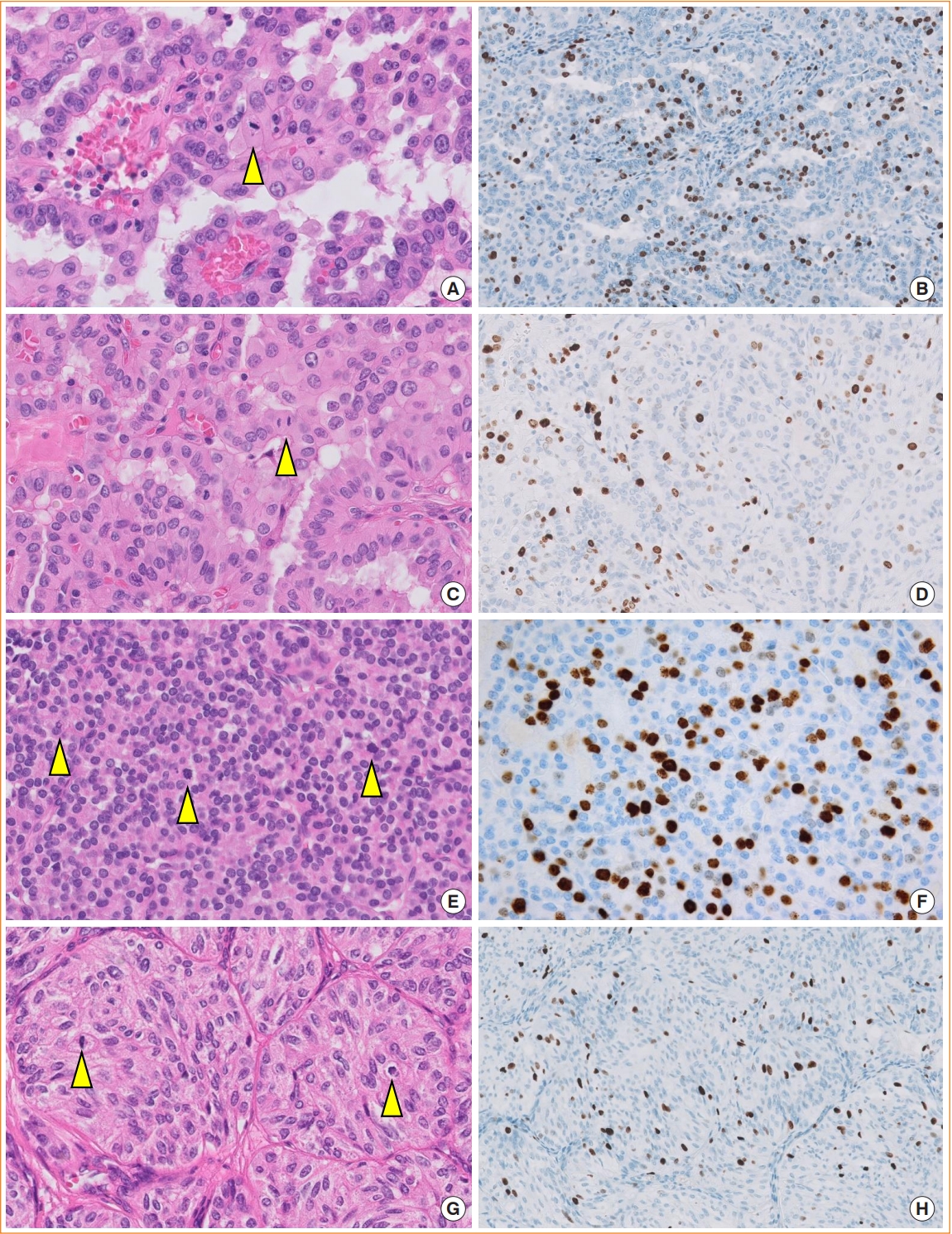
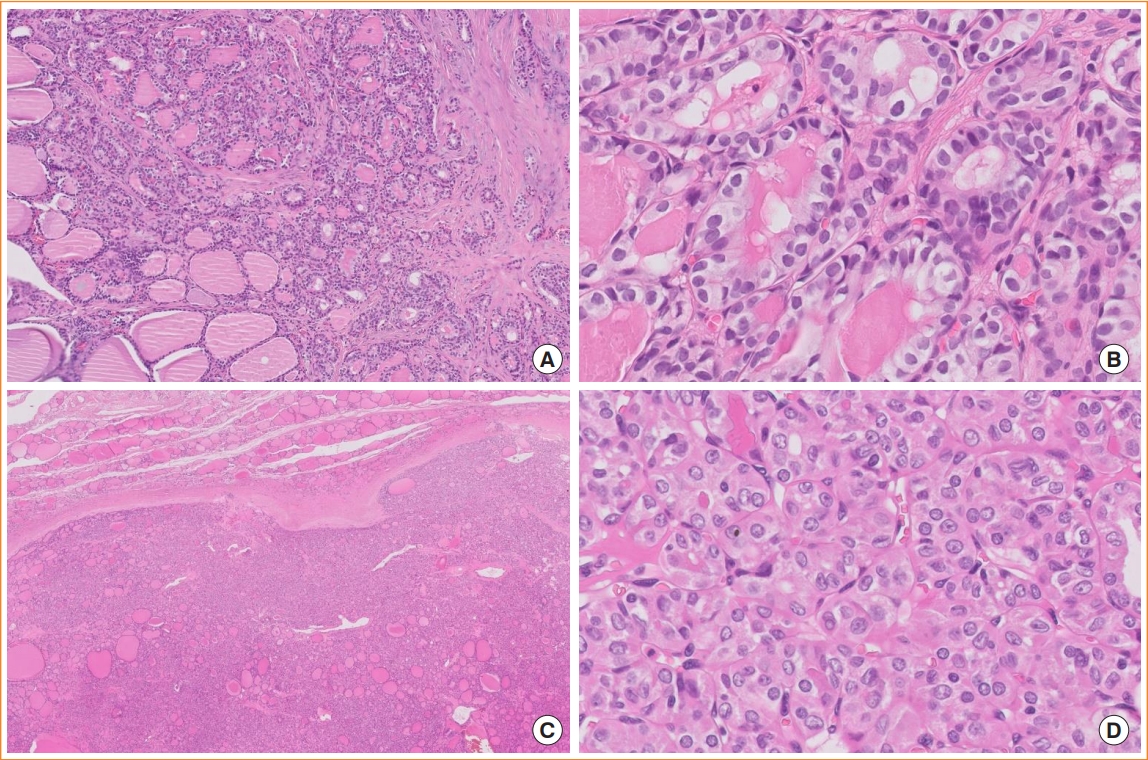
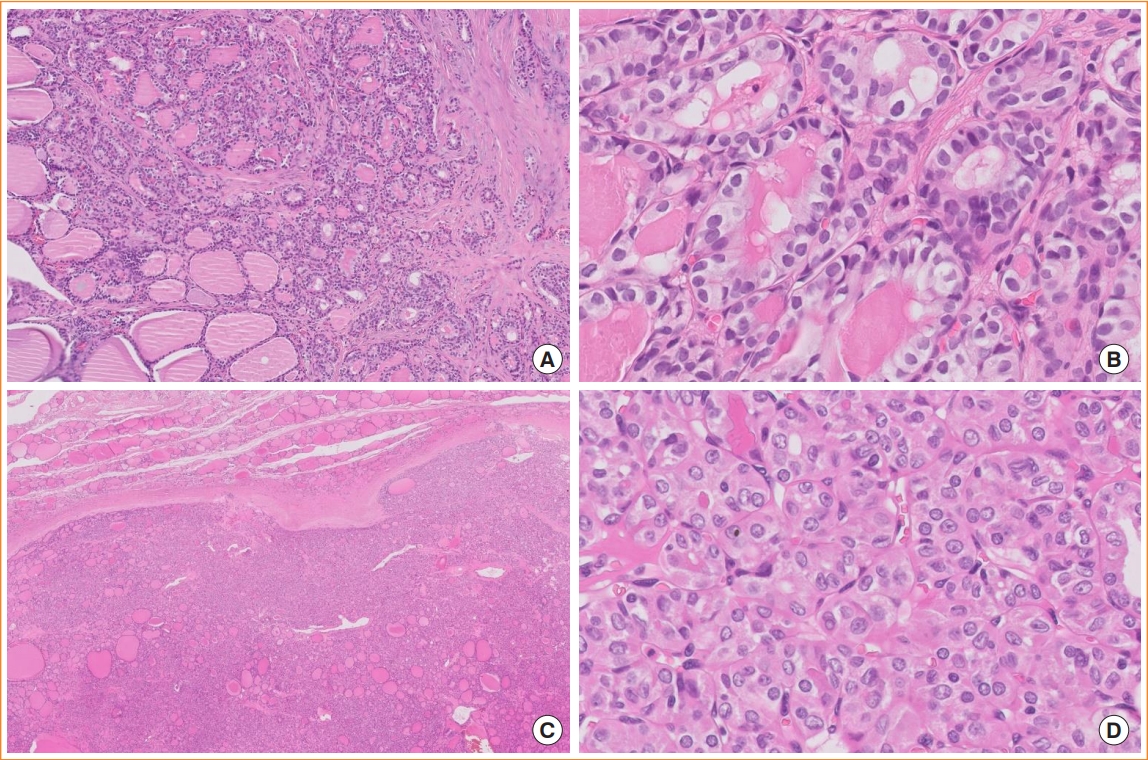
Fig. 4.
Increased mitotic activity and Ki67 index in high-grade thyroid cancers. Differentiated high-grade thyroid carcinomas can arise from hobnail papillary thyroid carcinoma (A, hematoxylin and eosin [H&E] stain, digital zoom ×100; B), tall cell papillary thyroid carcinoma (C, H&E stain, digital zoom ×100; D), and follicular thyroid carcinoma (E, H&E stain, digital zoom ×100; F). Immunohistochemical stains for Ki67 show proliferation index ≥5% (B, D, F; digital zoom ×40). High-grade medullary thyroid carcinoma shows mitotic count ≥5 per 2 mm2 (G, H&E stain, digital zoom ×100) and Ki67 proliferation index ≥5% (H, digital zoom ×40). Arrowheads indicate mitotic tumor cells.
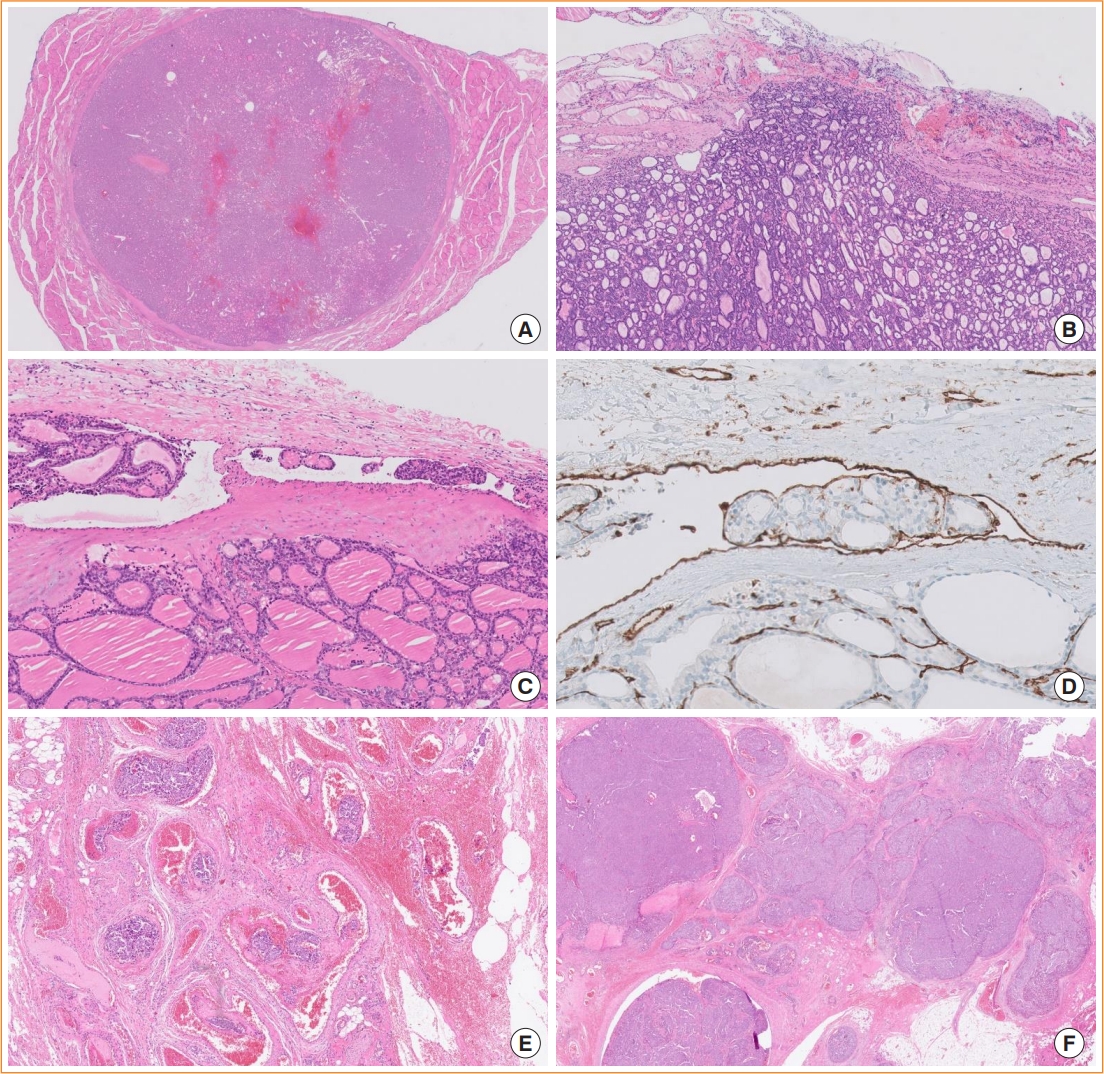
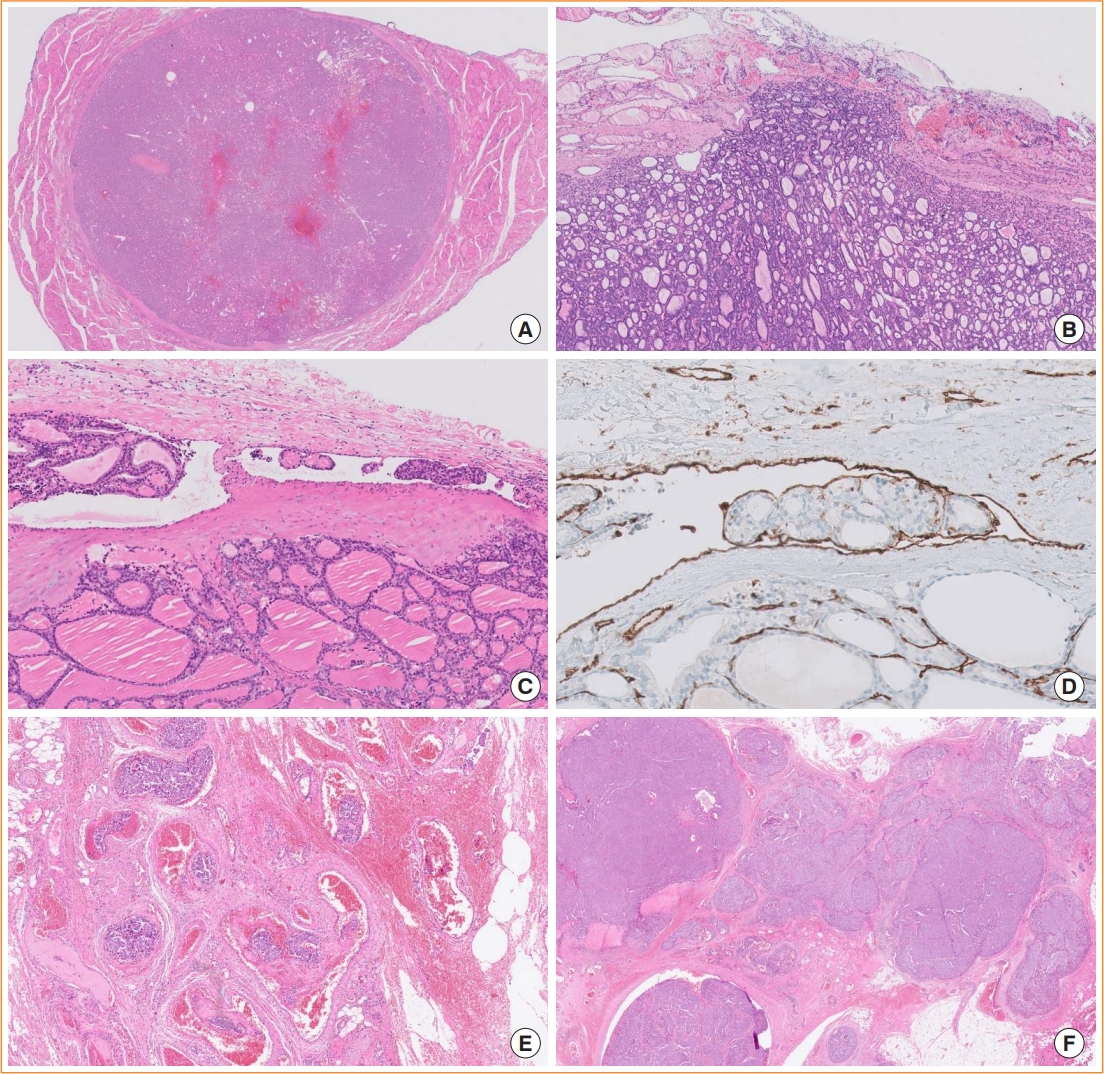
Fig. 5.
Subclassification of encapsulated follicular-derived thyroid tumors. Tumors with a non-invasive encapsulated follicular pattern include follicular adenoma and non-invasive follicular thyroid neoplasm with papillary-like nuclear features. (A) A follicular adenoma is shown (hematoxylin and eosin [H&E] stain, digital zoom ×1). (B) The minimally invasive subtype of follicular thyroid carcinoma has a tumor capsular invasion only (H&E stain, digital zoom ×10). (C) The encapsulated angioinvasive subtype is a cancer with vascular invasion regardless of capsular invasion status (H&E stain, digital zoom ×10). (D) CD31 immunostaining highlights endothelial-lined tumor emboli within the vessel (digital zoom ×40). (E) Extensive vascular invasion with ≥4 foci in extrathyroidal fibroadipose tissue is shown (H&E stain, digital zoom ×20). (F) The widely invasive subtype shows obliteration of the tumor capsule and invasion into extrathyroidal soft tissue (H&E stain, digital zoom ×10).
Fig. 6.
Follicular subtypes of papillary thyroid carcinoma (PTC). (A) Infiltrative follicular PTC shows an ill-defined infiltrative margin, follicular growth, and fibrotic stroma (digital zoom ×10). (B) Tumor cells have well-developed PTC nuclear features (digital zoom ×100). (C) Invasive encapsulated follicular variant PTC, which is now considered a separate entity and not a PTC subtype, invades through the fibrous capsule and shows a predominant follicular growth pattern (digital zoom ×10). (D) The nuclear features of invasive encapsulated follicular variant PTC are less developed than those of infiltrative follicular PTC; that is, the nuclei are rounder and more uniform (digital zoom ×100).
Fig. 7.
Tall cell and hobnail subtypes of papillary thyroid carcinoma (PTC) and encapsulated classic PTC with hobnail-like morphology. (A) Tall cell PTC shows an elongated and closely packed papillary pattern (hematoxylin and eosin [H&E] stain, digital zoom ×20). (B) The height of tumor cells is at least three times greater than their width (H&E stain, digital zoom ×100). Tumor cells have abundant eosinophilic cytoplasm and distinct cell membranes. (C) Hobnail PTC has papillary or micropapillary structures (H&E stain, digital zoom ×20). (D) Hobnail cells show enlarged hyperchromatic nuclei with reverse polarity (H&E stain, digital zoom ×100). (E) Encapsulated classic PTC shows cystic spaces and papillae lined with tumor cells having hobnail-like morphology (H&E stain, digital zoom ×20). (F) The papillary structure shows hyalinized and edematous stroma and cells with hobnailing cytomorphology (H&E stain, digital zoom ×100). The nuclear features look similar to those of classic PTC. These histologic findings are associated with ischemic and degenerative changes, and should not be diagnosed as hobnail PTC, which is an aggressive subtype.
Table 1.
Tumors of the Thyroid Gland in the 2022 WHO Classification of Endocrine and Neuroendocrine Tumors
Classification
ICD-O
ICD-11
1. Developmental abnormalities
Thyroglossal duct cyst
None
DA05.Y
Other congenital thyroid abnormalities
None
5A0Y
2. Follicular cell-derived neoplasms
Benign tumors
Thyroid follicular nodular disease
None
5A01.2
Follicular thyroid adenoma
8290/0
2F37.Y & XH0LM0
Follicular thyroid adenoma with papillary architecture
8330/0
2F37.Y & XH0LM0
Oncocytic adenoma of the thyroid
8290/0
2F37.Y & XH5SM2
Low risk neoplasms
Non-invasive follicular thyroid neoplasm with papillary-like nuclear features
8349/1
2F9A & XA8RK3
Thyroid tumors of uncertain malignant potential
Follicular tumor of uncertain malignant potential
8335/1
2F9A & XA8RK3
Well-differentiated tumor of uncertain malignant potential
4. Mixed medullary and follicular cell-derived carcinomas
Mixed medullary and follicular cell-derived thyroid carcinoma
Mixed medullary-follicular carcinoma
8346/3
2D10.Y & XH7DG7
Mixed medullary-papillary carcinoma
8347/3
2D10.Y & XH7DG7
5. Salivary gland-type carcinomas of the thyroid
Mucoepidermoid carcinoma of the thyroid
8430/3
2D10.Y & XH1J36
Secretory carcinoma of salivary gland type
8502/3
2D10.Y & XH44J4
6. Thyroid tumors of uncertain histogenesis
Sclerosing mucoepidermoid carcinoma with eosinophilia
8430/3
2D10.Y & XH1J36
Cribriform morular thyroid carcinoma
8201/3
2D10.Y & XH1YZ3
7. Thymic tumors within the thyroid
Thymoma family
Spindle epithelial tumor with thymus-like elements
8588/3
2D10.Y & XH6ZG8
Thymic carcinoma family
Intrathyroidal thymic carcinoma
8589/3
2C27.0
8. Embryonal thyroid neoplasms
Thyroblastoma
None
2D10.Y
WHO, World Health Organization; ICD-O, International Classification of Diseases for Oncology; ICD-11, International Classification of Diseases 11th Revision.
Table 2.
Major Revisions to the Classification and Nomenclature of Thyroid Tumors
a An anaplastic thyroid carcinoma component should not be seen. Thyroid tumors with mixed histologic patterns should be classified according to their least differentiated component and highest grade;
b The Ki67 proliferation index is not required for diagnosing poorly differentiated thyroid carcinoma and differentiated high-grade thyroid carcinoma, but these tumors usually have a Ki67 index of 10% to 30%;
c High-grade cancers have at least one of the three high-grade features;
d Low-grade cancers have mitotic count <5 per 2 mm2, no tumor necrosis, and Ki67 proliferation index <5%.
Table 4.
Differential Diagnosis of Thyroid Carcinomas of the Salivary Gland Type and Uncertain Histogenesis
Salivary gland type
Uncertain histogenesis
MEC
SC
SMECE
CMTC
Pathogenesis
MAML2 rearrangement (CRTC1::MAML2 fusion)
ETV6 translocations (ETV6::NTRK3 fusion)
MET hyperploidy, point mutations in APC, NTRK3, and NF1
1. Lloyd RV, Osamura RY, Kloppel G, Rosai J. WHO classification of tumours of endocrine organs; 4th ed. Lyon: International Agency for Research on Cancer (IARC); 2017. p. 65–91.
2. Mete O. Special issue on the 2022 WHO classification of endocrine and neuroendocrine tumors: a new primer for endocrine pathology practice. Endocr Pathol 2022;33:1–2.ArticlePubMedPMCPDF
3. Bai Y, Kakudo K, Jung CK. Updates in the pathologic classification of thyroid neoplasms: a review of the World Health Organization classification. Endocrinol Metab (Seoul) 2020;35:696–715.ArticlePubMedPMCPDF
4. Kakudo K, Bychkov A, Bai Y, Li Y, Liu Z, Jung CK. The new 4th edition World Health Organization classification for thyroid tumors, Asian perspectives. Pathol Int 2018;68:641–64.ArticlePubMedPDF
5. WHO Classification of Tumours Editorial Board. Endocrine and neuroendocrine tumours [Internet]. Lyon: International Agency for Research on Cancer; 2022 [cited 2022 Sep 19]. Available from: https://tumourclassification.iarc.who.int/chapters/36.
6. Baloch ZW, Asa SL, Barletta JA, Ghossein RA, Juhlin CC, Jung CK, et al. Overview of the 2022 WHO classification of thyroid neoplasms. Endocr Pathol 2022;33:27–63.ArticlePubMedPDF
7. Cancer Genome Atlas Research Network. Integrated genomic characterization of papillary thyroid carcinoma. Cell 2014;159:676–90.PubMedPMC
8. Yoo SK, Lee S, Kim SJ, Jee HG, Kim BA, Cho H, et al. Comprehensive analysis of the transcriptional and mutational landscape of follicular and papillary thyroid cancers. PLoS Genet 2016;12:e1006239.ArticlePubMedPMC
9. Asa SL, Mete O. Oncocytic change in thyroid pathology. Front Endocrinol (Lausanne) 2021;12:678119.ArticlePubMedPMC
10. Bruford EA, Antonescu CR, Carroll AJ, Chinnaiyan A, Cree IA, Cross NC, et al. HUGO Gene Nomenclature Committee (HGNC) recommendations for the designation of gene fusions. Leukemia 2021;35:3040–3.ArticlePubMedPMCPDF
11. Rivera M, Ricarte-Filho J, Knauf J, Shaha A, Tuttle M, Fagin JA, et al. Molecular genotyping of papillary thyroid carcinoma follicular variant according to its histological subtypes (encapsulated vs infiltrative) reveals distinct BRAF and RAS mutation patterns. Mod Pathol 2010;23:1191–200.ArticlePubMedPMCPDF
12. Kim TH, Lee M, Kwon AY, Choe JH, Kim JH, Kim JS, et al. Molecular genotyping of the non-invasive encapsulated follicular variant of papillary thyroid carcinoma. Histopathology 2018;72:648–61.ArticlePubMedPDF
13. Lee SR, Jung CK, Kim TE, Bae JS, Jung SL, Choi YJ, et al. Molecular genotyping of follicular variant of papillary thyroid carcinoma correlates with diagnostic category of fineneedle aspiration cytology: values of RAS mutation testing. Thyroid 2013;23:1416–22.ArticlePubMedPMC
14. Jung CK, Kim Y, Jeon S, Jo K, Lee S, Bae JS. Clinical utility of EZH1 mutations in the diagnosis of follicular-patterned thyroid tumors. Hum Pathol 2018;81:9–17.ArticlePubMed
15. Jung CK, Bychkov A, Song DE, Kim JH, Zhu Y, Liu Z, et al. Molecular correlates and nuclear features of encapsulated follicular-patterned thyroid neoplasms. Endocrinol Metab (Seoul) 2021;36:123–33.ArticlePubMedPMCPDF
16. Cree IA, Tan PH, Travis WD, Wesseling P, Yagi Y, White VA, et al. Counting mitoses: SI(ze) matters! Mod Pathol 2021;34:1651–7.ArticlePubMedPMCPDF
17. Hellgren LS, Stenman A, Paulsson JO, Hoog A, Larsson C, Zedenius J, et al. Prognostic utility of the Ki-67 labeling index in follicular thyroid tumors: a 20-year experience from a tertiary thyroid center. Endocr Pathol 2022;33:231–42.ArticlePubMedPMCPDF
18. Cree IA. From counting mitoses to Ki67 assessment: technical pitfalls in the new WHO classification of endocrine and neuroendocrine tumors. Endocr Pathol 2022;33:3–5.ArticlePubMedPDF
19. Xu B, Fuchs TL, Ahmadi S, Alghamdi M, Alzumaili B, Bani MA, et al. International medullary thyroid carcinoma grading system: a validated grading system for medullary thyroid carcinoma. J Clin Oncol 2022;40:96–104.ArticlePubMed
20. Calebiro D, Grassi ES, Eszlinger M, Ronchi CL, Godbole A, Bathon K, et al. Recurrent EZH1 mutations are a second hit in autonomous thyroid adenomas. J Clin Invest 2016;126:3383–8.ArticlePubMedPMC
21. Cho U, Mete O, Kim MH, Bae JS, Jung CK. Molecular correlates and rate of lymph node metastasis of non-invasive follicular thyroid neoplasm with papillary-like nuclear features and invasive follicular variant papillary thyroid carcinoma: the impact of rigid criteria to distinguish non-invasive follicular thyroid neoplasm with papillary-like nuclear features. Mod Pathol 2017;30:810–25.ArticlePubMedPDF
22. Nikiforov YE, Baloch ZW, Hodak SP, Giordano TJ, Lloyd RV, Seethala RR, et al. Change in diagnostic criteria for noninvasive follicular thyroid neoplasm with papillarylike nuclear features. JAMA Oncol 2018;4:1125–6.ArticlePubMedPMC
23. Xu B, Serrette R, Tuttle RM, Alzumaili B, Ganly I, Katabi N, et al. How many papillae in conventional papillary carcinoma?: a clinical evidence-based pathology study of 235 unifocal encapsulated papillary thyroid carcinomas, with emphasis on the diagnosis of noninvasive follicular thyroid neoplasm with papillary-like nuclear features. Thyroid 2019;29:1792–803.ArticlePubMedPMC
24. Nikiforov YE, Seethala RR, Tallini G, Baloch ZW, Basolo F, Thompson LD, et al. Nomenclature revision for encapsulated follicular variant of papillary thyroid carcinoma: a paradigm shift to reduce overtreatment of indolent tumors. JAMA Oncol 2016;2:1023–9.ArticlePubMedPMC
25. Xu B, Reznik E, Tuttle RM, Knauf J, Fagin JA, Katabi N, et al. Outcome and molecular characteristics of non-invasive encapsulated follicular variant of papillary thyroid carcinoma with oncocytic features. Endocrine 2019;64:97–108.ArticlePubMedPMCPDF
26. Xu B, Farhat N, Barletta JA, Hung YP, Biase D, Casadei GP, et al. Should subcentimeter non-invasive encapsulated, follicular variant of papillary thyroid carcinoma be included in the noninvasive follicular thyroid neoplasm with papillary-like nuclear features category? Endocrine 2018;59:143–50.ArticlePubMedPMCPDF
27. Ito Y, Hirokawa M, Miyauchi A, Higashiyama T, Kihara M, Miya A. Prognostic significance of the proportion of tall cell components in papillary thyroid carcinoma. World J Surg 2017;41:742–7.ArticlePubMedPDF
28. Wong KS, Chen TY, Higgins SE, Howitt BE, Lorch JH, Alexander EK, et al. A potential diagnostic pitfall for hobnail variant of papillary thyroid carcinoma. Histopathology 2020;76:707–13.ArticlePubMedPDF
29. Cameselle-Teijeiro JM, Eloy C, Sobrinho-Simoes M. Pitfalls in challenging thyroid tumors: emphasis on differential diagnosis and ancillary biomarkers. Endocr Pathol 2020;31:197–217.ArticlePubMedPMCPDF
30. Cho J, Shin JH, Hahn SY, Oh YL. Columnar cell variant of papillary thyroid carcinoma: ultrasonographic and clinical differentiation between the indolent and aggressive types. Korean J Radiol 2018;19:1000–5.ArticlePubMedPMCPDF
31. Chen JH, Faquin WC, Lloyd RV, Nose V. Clinicopathological and molecular characterization of nine cases of columnar cell variant of papillary thyroid carcinoma. Mod Pathol 2011;24:739–49.ArticlePubMedPDF
32. Lam AK. Squamous cell carcinoma of thyroid: a unique type of cancer in World Health Organization Classification. Endocr Relat Cancer 2020;27:R177–92.ArticlePubMed
33. Lai WA, Hang JF, Liu CY, Bai Y, Liu Z, Gu H, et al. PAX8 expression in anaplastic thyroid carcinoma is less than those reported in early studies: a multi-institutional study of 182 cases using the monoclonal antibody MRQ-50. Virchows Arch 2020;476:431–7.ArticlePubMedPDF
34. Chambers MA, Sadow PM, Kerr DA. Squamous differentiation in the thyroid: metaplasia, neoplasia, or bystander? Int J Surg Pathol 2022;30:385–92.ArticlePubMedPDF
35. Ito Y, Miyauchi A, Nakamura Y, Miya A, Kobayashi K, Kakudo K. Clinicopathologic significance of intrathyroidal epithelial thymoma/carcinoma showing thymus-like differentiation: a collaborative study with Member Institutes of The Japanese Society of Thyroid Surgery. Am J Clin Pathol 2007;127:230–6.ArticlePubMed
36. Saliba M, Mohanty AS, Ho AL, Drilon A, Dogan S. Secretory carcinoma of the thyroid in a 49-year-old man treated with larotrectinib: protracted clinical course of disease despite the high-grade histologic features. Head Neck Pathol 2022;16:612–20.ArticlePubMedPMCPDF
37. Tirado Y, Williams MD, Hanna EY, Kaye FJ, Batsakis JG, El-Naggar AK. CRTC1/MAML2 fusion transcript in high grade mucoepidermoid carcinomas of salivary and thyroid glands and Warthin’s tumors: implications for histogenesis and biologic behavior. Genes Chromosomes Cancer 2007;46:708–15.ArticlePubMed
38. Shah AA, La Fortune K, Miller C, Mills SE, Baloch Z, LiVolsi V, et al. Thyroid sclerosing mucoepidermoid carcinoma with eosinophilia: a clinicopathologic and molecular analysis of a distinct entity. Mod Pathol 2017;30:329–39.ArticlePubMedPMCPDF
39. Agaimy A, Togel L, Stoehr R, Meidenbauer N, Semrau S, Hartmann A, et al. NSD3-NUTM1-rearranged carcinoma of the median neck/thyroid bed developing after recent thyroidectomy for sclerosing mucoepidermoid carcinoma with eosinophilia: report of an extraordinary case. Virchows Arch 2021;479:1095–9.ArticlePubMedPMCPDF
40. Wiles AB, Kraft AO, Mueller SM, Powers CN. Sclerosing mucoepidermoid carcinoma with eosinophilia of the thyroid: case report of a rare lesion with novel genetic mutation. Diagn Cytopathol 2019;47:589–93.ArticlePubMedPDF
41. Hunt JL, LiVolsi VA, Barnes EL. p63 expression in sclerosing mucoepidermoid carcinomas with eosinophilia arising in the thyroid. Mod Pathol 2004;17:526–9.ArticlePubMedPDF
42. Werner RG, Langlouis-Gau H, Walz F, Allgaier H, Hoffmann H. Validation of biotechnological production processes. Arzneimittelforschung 1988;38:855–62.PubMed
43. Noor M, Russell DK, Israel AK, Lott Limbach A. Thyroid sclerosing mucoepidermoid carcinoma with eosinophilia in conjunction with parotid basal cell adenoma: cytologic, histologic, and molecular features. Diagn Cytopathol 2021;49:E262–8.ArticlePubMedPDF
44. Cameselle-Teijeiro JM, Peteiro-Gonzalez D, Caneiro-Gomez J, Sanchez-Ares M, Abdulkader I, Eloy C, et al. Cribriform-morular variant of thyroid carcinoma: a neoplasm with distinctive phenotype associated with the activation of the WNT/β-catenin pathway. Mod Pathol 2018;31:1168–79.ArticlePubMedPDF
45. Boyraz B, Sadow PM, Asa SL, Dias-Santagata D, Nose V, Mete O. Cribriform-morular thyroid carcinoma is a distinct thyroid malignancy of uncertain cytogenesis. Endocr Pathol 2021;32:327–35.ArticlePubMedPMCPDF
46. Nose V. Familial thyroid cancer: a review. Mod Pathol 2011;24 Suppl 2:S19–33.PubMed
47. Guilmette J, Nose V. Hereditary and familial thyroid tumours. Histopathology 2018;72:70–81.ArticlePubMedPDF
48. Rooper LM, Bynum JP, Miller KP, Lin MT, Gagan J, Thompson LD, et al. Recurrent DICER1 hotspot mutations in malignant thyroid gland teratomas: molecular characterization and proposal for a separate classification. Am J Surg Pathol 2020;44:826–33.PubMed
49. Agaimy A, Witkowski L, Stoehr R, Cuenca JC, GonzalezMuller CA, Brutting A, et al. Malignant teratoid tumor of the thyroid gland: an aggressive primitive multiphenotypic malignancy showing organotypical elements and frequent DICER1 alterations-is the term “thyroblastoma” more appropriate? Virchows Arch 2020;477:787–98.ArticlePubMedPMCPDF
50. Yang J, Sarita-Reyes C, Kindelberger D, Zhao Q. A rare malignant thyroid carcinosarcoma with aggressive behavior and DICER1 gene mutation: a case report with literature review. Thyroid Res 2018;11:11.ArticlePubMedPMCPDF
51. Wong KS, Dong F, Telatar M, Lorch JH, Alexander EK, Marqusee E, et al. Papillary thyroid carcinoma with highgrade features versus poorly differentiated thyroid carcinoma: an analysis of clinicopathologic and molecular features and outcome. Thyroid 2021;31:933–40.ArticlePubMed
52. Xu B, David J, Dogan S, Landa I, Katabi N, Saliba M, et al. Primary high-grade non-anaplastic thyroid carcinoma: a retrospective study of 364 cases. Histopathology 2022;80:322–37.ArticlePubMedPDF
53. Rivera M, Ghossein RA, Schoder H, Gomez D, Larson SM, Tuttle RM. Histopathologic characterization of radioactive iodine-refractory fluorodeoxyglucose-positron emission tomography-positive thyroid carcinoma. Cancer 2008;113:48–56.ArticlePubMed
Figure & Data
References
Citations
Citations to this article as recorded by
Tumeurs de la thyroïde : nouveautés de la classification OMS 2022 Serge Guyétant, Myriam Decaussin Petrucci, Emmanuelle Leteurtre Annales de Pathologie.2024; 44(1): 5. CrossRef
Diagnostic Performance of [18F]TFB PET/CT Compared with Therapeutic Activity [131I]Iodine SPECT/CT and [18F]FDG PET/CT in Recurrent Differentiated Thyroid Carcinoma David Ventura, Matthias Dittmann, Florian Büther, Michael Schäfers, Kambiz Rahbar, Daniel Hescheler, Michael Claesener, Philipp Schindler, Burkhard Riemann, Robert Seifert, Wolfgang Roll Journal of Nuclear Medicine.2024; 65(2): 192. CrossRef
Clinicopathological features of differentiated thyroid carcinoma as predictors of the effects of radioactive iodine therapy Wen Liu, Beibei Jiang, Jingli Xue, Ruijing Liu, Yuqing Wei, Peifeng Li Annals of Diagnostic Pathology.2024; 69: 152243. CrossRef
Management of aggressive variants of papillary thyroid cancer Ying Ki Lee, Aleix Rovira, Paul V. Carroll, Ricard Simo Current Opinion in Otolaryngology & Head & Neck Surgery.2024; 32(2): 125. CrossRef
Artificial Intelligence Detected the Relationship Between Nuclear Morphological Features and Molecular Abnormalities of Papillary Thyroid Carcinoma Toui Nishikawa, Ibu Matsuzaki, Ayata Takahashi, Iwamoto Ryuta, Fidele Yambayamba Musangile, Kanako Sagan, Mizuki Nishikawa, Yurina Mikasa, Yuichi Takahashi, Fumiyoshi Kojima, Shin-ichi Murata Endocrine Pathology.2024; 35(1): 40. CrossRef
Review of the 2023 World Congress on Thyroid Cancer (WCTC 2023, London): is there light at the end of the tunnel for patients with neglected cancer? S.M. Cherenko INTERNATIONAL JOURNAL OF ENDOCRINOLOGY (Ukraine).2024; 19(8): 609. CrossRef
Molecular Alterations and Comprehensive Clinical Management of Oncocytic Thyroid Carcinoma Lindsay A. Bischoff, Ian Ganly, Laura Fugazzola, Erin Buczek, William C. Faquin, Bryan R. Haugen, Bryan McIver, Caitlin P. McMullen, Kate Newbold, Daniel J. Rocke, Marika D. Russell, Mabel Ryder, Peter M. Sadow, Eric Sherman, Maisie Shindo, David C. Shonk JAMA Otolaryngology–Head & Neck Surgery.2024; 150(3): 265. CrossRef
Malignancy in a Solitary Thyroid Nodule: A Retrospective Histopathological Evaluation Hassan Alzahrani International Journal of General Medicine.2024; Volume 17: 135. CrossRef
Pathologie thyroïdienne. Actualités et problèmes pratiques. Introduction Serge Guyétant Annales de Pathologie.2024; 44(2): 90. CrossRef
Diagnostic implication of thyroid spherules for cytological diagnosis of thyroid nodules Heeseung Sohn, Kennichi Kakudo, Chan Kwon Jung Cytopathology.2024; 35(3): 383. CrossRef
Aggressive Primary Thyroid Mucoepidermoid Carcinoma with Extensive Pulmonary Involvement Marius Mitrache, Dana Terzea, Anca Sirbu, Simona Fica Biomedicines.2024; 12(2): 285. CrossRef
Unravelling the role of long non-coding RNAs in modulating the Hedgehog pathway in cancer Shailendra Singh Chandel, Anurag Mishra, Gaurav Dubey, Ravindra Pal Singh, Mithilesh Singh, Mohit Agarwal, Himmat Singh Chawra, Neelima Kukreti Pathology - Research and Practice.2024; 254: 155156. CrossRef
Hürthle cell (Oncocytic) carcinoma – Is hemithyroidectomy enough? Taylor O. Julsrud, Trenton R. Foster, Robert A. Vierkant, Melanie L. Lyden, Travis J. McKenzie, Mabel Ryder, Benzon M. Dy Surgical Oncology Insight.2024; 1(1): 100010. CrossRef
Échographie des carcinomes thyroïdiens différenciés de souche folliculaire P.Y. Marcy, M. Tassart, J.G. Marchand, J. Sanglier, A. Bizeau, E. Ghanassia Journal d'imagerie diagnostique et interventionnelle.2024; 7(2): 54. CrossRef
Differentiating BRAF V600E- and RAS-like alterations in encapsulated follicular patterned tumors through histologic features: a validation study Chankyung Kim, Shipra Agarwal, Andrey Bychkov, Jen-Fan Hang, Agnes Stephanie Harahap, Mitsuyoshi Hirokawa, Kennichi Kakudo, Somboon Keelawat, Chih-Yi Liu, Zhiyan Liu, Truong Phan-Xuan Nguyen, Chanchal Rana, Huy Gia Vuong, Yun Zhu, Chan Kwon Jung Virchows Archiv.2024;[Epub] CrossRef
Cas no5. High-grade Tall cell papillary carcinoma Myriam Decaussin-Petrucci Annales de Pathologie.2024; 44(2): 114. CrossRef
Current and future of immunotherapy for thyroid cancer based on bibliometrics and clinical trials Ke Wang, Ying Zhang, Yang Xing, Hong Wang, Minghua He, Rui Guo Discover Oncology.2024;[Epub] CrossRef
Cas no6. Anaplastic thyroid carcinoma, epidermoid subtype Myriam Decaussin-Petrucci Annales de Pathologie.2024; 44(2): 120. CrossRef
Papillary Thyroid Carcinoma With Lymphoepithelial Features and Lacking Association With Epstein-Barr Virus (EBV): A Rare Case Ahmed Bendari, Saroja Devi Geetha, Reham Al-Refai, Xuelin Zhong, Sunder Sham, Manju Harshan Cureus.2024;[Epub] CrossRef
Clinical and morphological features and unsolved issues in diagnosis of aggressive forms of papillary thyroid carcinoma Denis V. Korotovsky, Sergey V. Sergiiko, Sergey A. Lukyanov Perm Medical Journal.2024; 41(1): 90. CrossRef
Finding possible diagnostic markers for differentiating benign and malignant thyroid tumors on example investigate of rheological properties1 I. Javakhishvili, T. Sanikidze, K. Mardaleishvili, N. Momtselidze, T. Urdulashvili, M. Mantskava, L. Prantl, F. Jung Clinical Hemorheology and Microcirculation.2024; : 1. CrossRef
Unraveling the Significance of DGCR8 and miRNAs in Thyroid Carcinoma Lia Rodrigues, Arnaud Da Cruz Paula, Paula Soares, João Vinagre Cells.2024; 13(7): 561. CrossRef
Management of Poorly Differentiated Thyroid Cancer and Differentiated High-Grade Thyroid Carcinoma Iram S. Alam, Kepal N. Patel Surgical Clinics of North America.2024;[Epub] CrossRef
What’s new in thyroid pathology 2024: updates from the new WHO classification and bethesda system Andrey Bychkov, Chan Kwon Jung Journal of Pathology and Translational Medicine.2024; 58(2): 98. CrossRef
Ultrasound–Histopathological Presentation of Thyroid and Ovary Lesions in Adolescent Patients with DICER1 Syndrome: Case Reports and Literature Overview Dominika Januś, Monika Kujdowicz, Konrad Kaleta, Kamil Możdżeń, Jan Radliński, Anna Taczanowska-Niemczuk, Aleksandra Kiszka-Wiłkojć, Marcin Maślanka, Wojciech Górecki, Jerzy B. Starzyk Children.2024; 11(4): 403. CrossRef
Surgical treatment of solid variant of papillary thyroid carcinoma: Fifteen-year experience of a tertiary center Katarina Tausanović, Marina Stojanović, Milan Jovanović, Boban Stepanović, Jovan Ilić, Sara Ivaniš, Vladan Živaljević Medicinska istrazivanja.2024; 57(1): 121. CrossRef
Critical appraisal of the WHO 2022 classification of thyroid cancer Mithraa Devi Sekar, Debasis Gochhait, Sadishkumar Kamalanathan Thyroid Research and Practice.2024; 20(1): 8. CrossRef
Patterns in the Reporting of Aggressive Histologic Subtypes in Papillary Thyroid Cancer Yeon J. Lee, Caitlin E. Egan, Jacques A. Greenberg, Teagan Marshall, Abhinay Tumati, Brendan M. Finnerty, Toni Beninato, Rasa Zarnegar, Thomas J. Fahey, Minerva A. Romero Arenas Journal of Surgical Research.2024; 298: 325. CrossRef
Update on C-Cell Neuroendocrine Neoplasm: Prognostic and Predictive Histopathologic and Molecular Features of Medullary Thyroid Carcinoma Chan Kwon Jung, Shipra Agarwal, Jen-Fan Hang, Dong-Jun Lim, Andrey Bychkov, Ozgur Mete Endocrine Pathology.2023; 34(1): 1. CrossRef
The 5th edition of WHO classification of tumors of endocrine organs: changes in the diagnosis of follicular-derived thyroid carcinoma Fulvio Basolo, Elisabetta Macerola, Anello Marcello Poma, Liborio Torregrossa Endocrine.2023; 80(3): 470. CrossRef
Preoperative Risk Stratification of Follicular-patterned Thyroid Lesions on Core Needle Biopsy by Histologic Subtyping and RAS Variant-specific Immunohistochemistry Meejeong Kim, Sora Jeon, Chan Kwon Jung Endocrine Pathology.2023; 34(2): 247. CrossRef
Ultrasound evolution of parenchymal changes in the thyroid gland with autoimmune thyroiditis in children prior to the development of papillary thyroid carcinoma – a follow-up study Dominika Januś, Monika Kujdowicz, Małgorzata Wójcik, Anna Taczanowska-Niemczuk, Aleksandra Kiszka-Wiłkojć, Wojciech Górecki, Jerzy B. Starzyk Frontiers in Endocrinology.2023;[Epub] CrossRef
Papillary thyroid carcinoma with aggressive fused follicular and solid growth pattern: A unique histological subtype with high‐grade malignancy? Shin‐ichi Murata, Ibu Matsuzaki, Mitsuo Kishimoto, Naomi Katsuki, Toshinori Onishi, Mitsuyoshi Hirokawa, Fumiyoshi Kojima Pathology International.2023; 73(5): 207. CrossRef
Multi-Omics and Management of Follicular Carcinoma of the Thyroid Thifhelimbilu Emmanuel Luvhengo, Ifongo Bombil, Arian Mokhtari, Maeyane Stephens Moeng, Demetra Demetriou, Claire Sanders, Zodwa Dlamini Biomedicines.2023; 11(4): 1217. CrossRef
Molecular Genetics of Diffuse Sclerosing Papillary Thyroid Cancer Meshael Alswailem, Balgees Alghamdi, Anwar Alotaibi, Abeer Aljomiah, Hindi Al-Hindi, Avaniyapuram Kannan Murugan, Mohamed Abouelhoda, Yufei Shi, Ali S Alzahrani The Journal of Clinical Endocrinology & Metabolism.2023; 108(9): e704. CrossRef
Multifunctional Phase-Transition Nanoparticles for Effective Targeted Sonodynamic-Gene Therapy Against Thyroid Papillary Carcinoma Shihui Guan, Dengke Teng, Hui Wang, Qimeihui Wang, Xi Zhen, Guoqing Sui, Yang Wang, Lingyu Zhu, Yuanqiang Lin, Dan Jiao, Feng Guo International Journal of Nanomedicine.2023; Volume 18: 2275. CrossRef
Utilizing Dynamic Risk Stratification in Patients With Tall Cell Variant Papillary Thyroid Cancer David Zimmer, Gilman Plitt, Brandon Prendes, Jamie Ku, Natalie Silver, Eric Lamarre, Emrullah Yilmaz, Jessica Geiger, Christian Nasr, Lea El Hage, Mario Skugor, Shauna Cambpell, Shlomo Koyfman, Jacob Miller, Neil Woody, Katherine Heiden, Nikhil Joshi, Tar The Laryngoscope.2023; 133(9): 2430. CrossRef
Ultrasound, laboratory and histopathological insights in diagnosing papillary thyroid carcinoma in a paediatric population: a single centre follow-up study between 2000-2022 Dominika Januś, Małgorzata Wójcik, Anna Taczanowska-Niemczuk, Aleksandra Kiszka-Wiłkojć, Monika Kujdowicz, Małgorzata Czogała, Wojciech Górecki, Jerzy B. Starzyk Frontiers in Endocrinology.2023;[Epub] CrossRef
Medullary Thyroid Carcinoma: A Single Institute Experience Sonal Trivedi, T. Salahuddin, Mohamed Taher Mithi, Priyank Rathod, Arpit Bandi, Shashank J. Pandya, Mohit Sharma, Shailesh Patel, Vikas Warikoo, Ketul Puj, Abhijeet Salunkhe, Keval Patel, Shivam Pandya Indian Journal of Otolaryngology and Head & Neck Surgery.2023; 75(4): 2884. CrossRef
FNAC (Fine needle aspiration cytology) and histopathological correlation and reclassification of thyroid neoplasm in accordance with WHO classification 2022 Fareeda Joshi, Shreya Hegde Indian Journal of Pathology and Oncology.2023; 10(2): 132. CrossRef
Papillary thyroid carcinoma associated with non‑functioning parathyroid carcinoma with Warthin's tumor of the parotid gland: A case report and brief literature review Ari Abdullah, Aras Qaradakhy, Yadgar Saeed, Abdulwahid Salih, Seema Karim, Osama Ali, Shko Hassan, Shalaw Nasraldeen, Shvan Mohammed, Fahmi Kakamad Medicine International.2023;[Epub] CrossRef
Warthin-like papillary thyroid carcinoma: a case report and comprehensive review of the literature Abdel Mouhaymen Missaoui, Fatma Hamza, Wafa Belabed, Manel Mellouli, Mohamed Maaloul, Slim Charfi, Issam Jardak, Tahya Sellami-Boudawara, Nabila Rekik, Mohamed Abid Frontiers in Endocrinology.2023;[Epub] CrossRef
Reevaluating diagnostic categories and associated malignancy risks in thyroid core needle biopsy Chan Kwon Jung Journal of Pathology and Translational Medicine.2023; 57(4): 208. CrossRef
Cancer Predisposition Syndromes and Thyroid Cancer: Keys for a Short Two-Way Street Ioana Balinisteanu, Monica-Cristina Panzaru, Lavinia Caba, Maria-Christina Ungureanu, Andreea Florea, Ana Maria Grigore, Eusebiu Vlad Gorduza Biomedicines.2023; 11(8): 2143. CrossRef
Deep learning prediction model for central lymph node metastasis in papillary thyroid microcarcinoma based on cytology Wenhao Ren, Yanli Zhu, Qian Wang, Yuntao Song, Zhihui Fan, Yanhua Bai, Dongmei Lin Cancer Science.2023; 114(10): 4114. CrossRef
Cytology and Histology of Thyroid Nodules: Exploring Novel Insights in the Molecular Era for Enhanced Patient Management Beatrix Cochand-Priollet, Zahra Maleki Current Oncology.2023; 30(8): 7753. CrossRef
Agrin is a novel oncogenic protein in thyroid cancer Anna Adamiok‑Ostrowska, Małgorzata Grzanka, Barbara Czarnocka Oncology Letters.2023;[Epub] CrossRef
Analysis of Pathological Features of Thyroid Carcinoma in the Western Yunnan 身吾 王 Advances in Clinical Medicine.2023; 13(10): 15820. CrossRef
Insight of novel biomarkers for papillary thyroid carcinoma through multiomics Wei Liu, Junkan Zhu, Zhen Wu, Yongxiang Yin, Qiao Wu, Yiming Wu, Jiaojiao Zheng, Cong Wang, Hongyan Chen, Talal Jamil Qazi, Jun Wu, Yuqing Zhang, Houbao Liu, Jingmin Yang, Daru Lu, Xumin Zhang, Zhilong Ai Frontiers in Oncology.2023;[Epub] CrossRef
Identification of NIFTP-Specific mRNA Markers for Reliable Molecular Diagnosis of Thyroid Tumors So-Yeon Lee, Jong-Lyul Park, Kwangsoon Kim, Ja Seong Bae, Jae-Yoon Kim, Seon-Young Kim, Chan Kwon Jung Endocrine Pathology.2023; 34(3): 311. CrossRef
Somatostatin Receptor Type 2 and Thyroid-Stimulating Hormone Receptor Expression in Oncocytic Thyroid Neoplasms: Implications for Prognosis and Treatment Andrea Gillis, Rui Zheng-Pywell, Chandler McLeod, Dezhi Wang, John M. Ness, Rachael Guenter, Jason Whitt, Tomas A. Prolla, Herbert Chen, Manuel Lora Gonzalez, Bart Rose, Ricardo V. Lloyd, Renata Jaskula-Sztul, Diana Lin Modern Pathology.2023; 36(12): 100332. CrossRef
Comparison of Treatment and Prognosis Between Follicular Variant
Papillary Thyroid Carcinoma and Classical Papillary Thyroid
Carcinoma Bing Zhang, Wenming Wu, Jinjing Liu, Zhou Liang, Liang Zong Hormone and Metabolic Research.2023; 55(12): 855. CrossRef
Sentinel lymph node mapping: current applications and future perspectives in thyroid carcinoma Isabella Merante Boschin, Loris Bertazza, Carla Scaroni, Caterina Mian, Maria Rosa Pelizzo Frontiers in Medicine.2023;[Epub] CrossRef
Utility of the Growth Differentiation Factor-15 in the Differential Diagnosis of Follicular-Patterned Lesions of the Thyroid on Cytopathologic and Histopathologic Samples Prasanna V Perumal, Neelaiah Siddaraju, Sunil K Saxena, Soundravally Rajendiran, Ramachandra V Bhat Cureus.2023;[Epub] CrossRef
Applications of machine and deep learning to thyroid cytology and histopathology: a review Greg Slabaugh, Luis Beltran, Hasan Rizvi, Panos Deloukas, Eirini Marouli Frontiers in Oncology.2023;[Epub] CrossRef
The Asian Thyroid Working Group, from 2017 to 2023 Kennichi Kakudo, Chan Kwon Jung, Zhiyan Liu, Mitsuyoshi Hirokawa, Andrey Bychkov, Huy Gia Vuong, Somboon Keelawat, Radhika Srinivasan, Jen-Fan Hang, Chiung-Ru Lai Journal of Pathology and Translational Medicine.2023; 57(6): 289. CrossRef
Simultaneous Occurrence of Medullary Thyroid Carcinoma and Papillary Thyroid Carcinoma: A Case Series with Literature Review Poupak Fallahi, Armando Patrizio, Giulio Stoppini, Giusy Elia, Francesca Ragusa, Sabrina Rosaria Paparo, Eugenia Balestri, Valeria Mazzi, Chiara Botrini, Gilda Varricchi, Salvatore Ulisse, Marco Ghionzoli, Alessandro Antonelli, Silvia Martina Ferrari Current Oncology.2023; 30(12): 10237. CrossRef
Construction and validation of a nomogram for predicting cervical lymph node metastasis in diffuse sclerosing variant of papillary thyroid carcinoma Xunyi Lin, Jiaxing Huo, Huan Zhang, Hang Su, Fenghua Zhang Langenbeck's Archives of Surgery.2023;[Epub] CrossRef
Canine follicular cell and medullary thyroid carcinomas: Immunohistochemical characterization Jana Jankovic, Eve Tièche, Martina Dettwiler, Kerstin Hahn, Stephanie Scheemaeker, Martin Kessler, Sylvie Daminet, Sven Rottenberg, Miguel Campos Veterinary Pathology.2023;[Epub] CrossRef
A 16-Year Single-Center Series of Trachea Resections for Locally Advanced Thyroid Carcinoma Julia I. Staubitz-Vernazza, Sina Schwind, Oana Lozan, Thomas J. Musholt Cancers.2023; 16(1): 163. CrossRef
Reprogramming of Cellular Metabolism and Its Therapeutic Applications in Thyroid Cancer Yuji Nagayama, Koichiro Hamada Metabolites.2022; 12(12): 1214. CrossRef
Developments to improve outcomes in thyroid surgery Thomas J. Musholt Innovative Surgical Sciences.2022; 7(3-4): 77. CrossRef
The relationship of the clinicopathological characteristics and treatment results of post-Chornobyl papillary thyroid microcarcinomas with the latency period and radiation exposure Tetiana Bogdanova, Serhii Chernyshov, Liudmyla Zurnadzhy, Tatiana I. Rogounovitch, Norisato Mitsutake, Mykola Tronko, Masahiro Ito, Michael Bolgov, Sergii Masiuk, Shunichi Yamashita, Vladimir A. Saenko Frontiers in Endocrinology.2022;[Epub] CrossRef

 Keypoint
Keypoint , Andrey Bychkov3, Kennichi Kakudo4
, Andrey Bychkov3, Kennichi Kakudo4 





 PubReader
PubReader ePub Link
ePub Link Cite
Cite