Articles
- Page Path
- HOME > Endocrinol Metab > Volume 34(4); 2019 > Article
-
Review ArticleIntraoperative Parathyroid Hormone Monitoring in the Surgical Management of Sporadic Primary Hyperparathyroidism
-
Zahra F. Khan
 , John I. Lew
, John I. Lew -
Endocrinology and Metabolism 2019;34(4):327-339.
DOI: https://doi.org/10.3803/EnM.2019.34.4.327
Published online: December 23, 2019
Division of Endocrine Surgery, DeWitt Daughtry Family Department of Surgery, University of Miami Leonard M. Miller School of Medicine, Miami, FL, USA.
- Corresponding author: John I. Lew. Division of Endocrine Surgery, DeWitt Daughtry Family Department of Surgery, Jackson Memorial Hospital, University of Miami Leonard M. Miller School of Medicine, CRB-Room 410P (M-875), 1120 NW 14th St, Miami, FL 33136, USA. Tel: +1-305-243-4444, Fax: +1-305-243-4221, JLew@med.miami.edu
Copyright © 2019 Korean Endocrine Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- ABSTRACT
- INTRODUCTION
- PARADIGM SHIFT OF OPERATIVE APPROACH TO FUNCTION
- CLINICAL MANIFESTATIONS OF SPHPT
- INDICATIONS FOR IPM GUIDED PARATHYROIDECTOMY
- IPM AND THE “MIAMI CRITERION”
- INTRAOPERATIVE PTH DYNAMICS
- APPLICATIONS OF IPM GUIDED PARATHYROIDECTOMY
- LONG TERM RESULTS OF IPM GUIDED PARATHYROIDECTOMY
- ADDITIONAL USES FOR THE INTRAOPERATIVE PTH ASSAY
- CONCLUSIONS
- Article information
- References
ABSTRACT
- Intraoperative parathyroid hormone monitoring (IPM) has been shown to be a useful adjunct during parathyroidectomy to ensure operative success at many specialized medical centers worldwide. Using the Miami or “>50% intraoperative PTH drop” criterion, IPM confirms the complete excision of all hyperfunctioning parathyroid tissue before the operation is finished, and helps guide the surgeon to identify additional hyperfunctioning parathyroid glands that may necessitate further extensive neck exploration when intraoperative parathyroid hormone (PTH) levels do not drop sufficiently. The intraoperative PTH assay is also used to differentiate parathyroid from non-parathyroid tissues during operations using fine needle aspiration samples and to lateralize the side of the neck harboring the hypersecreting parathyroid through differential jugular venous sampling when preoperative localization studies are negative or equivocal. The use of IPM underscores the recognition and understanding of sporadic primary hyperparathyroidism (SPHPT) as a disease of function rather than form, where the surgeon is better equipped to treat such patients with quantitative instead of qualitative information for durable long-term operative success. There has been a significant paradigm shift over the last 2 decades from conventional to focused parathyroidectomy guided by IPM. This approach has proven to be a safe and rapid operation requiring minimal dissection performed in an ambulatory setting for the treatment of SPHPT.
- Since the first parathyroidectomy performed in 1925 by Dr. Felix Mandl of Vienna, bilateral neck exploration (BNE) by an experienced surgeon has been the gold standard with operative success rates of >95% in patients with sporadic primary hyperparathyroidism (SPHPT) [1234]. Advanced and available imaging modalities such as sestamibi (MIBI) scintigraphy and/or high-resolution neck ultrasonography for the preoperative localization of abnormal parathyroid glands and the innovation of intact serum parathyroid hormone (PTH) measurement or intraoperative PTH monitoring (IPM) as a point-of-care test have become the cornerstones for focused or minimally invasive parathyroidectomy [56789]. Focused parathyroidectomy guided by IPM is a quantitative operative approach that allows the excision of an image-localized hypersecreting parathyroid gland without disturbing or visualizing the other normal functioning parathyroid glands in situ, and achieving operative success with rapid and minimal dissection.
- An important component of focused parathyroidectomy, the intraoperative PTH assay helps surgeons quantitatively determine the excision of all hyperfunctioning parathyroid tissue, and predict long-term operative success [56789]. Furthermore, in patients with multiglandular disease (MGD), the intraoperative measurement of PTH levels accurately identifies the underlying presence of additional hypersecreting parathyroid gland(s) and indicates if further neck exploration is required [1011]. Over the last 2 decades, the use of intraoperative PTH assays in the performance of focused or minimally invasive parathyroidectomy has supplanted traditional BNE for SPHPT as the standard approach at many specialized centers worldwide [1213].
- In 1987, Nussbaum et al. [14] described a novel method for measuring the intact (1-84) PTH molecule by using a 2-site antibody technique more sensitive and specific than previous assays. With its rapid rate of decay (half-life, 3 to 5 minutes), PTH can be quickly and quantitatively measured intraoperatively and predicts postoperative eucalcemia in patients after successful parathyroidectomy for SPHPT. In 1991, Irvin et al. [15161718] refined and applied this PTH assay intraoperatively, also known as IPM, to routine clinical practice in the surgical treatment of SPHPT at the University of Miami. Since 1996, rapid intraoperative PTH assays have become commercially available, and such surgical adjuncts are now utilized routinely by parathyroid surgeons [57891213]. This article reviews the current role of IPM in the surgical management of SPHPT.
INTRODUCTION
- The rapid intraoperative PTH measurement in plasma and tissue has changed the understanding and surgical management of SPHPT, which is the result of autonomous PTH hypersecretion by one or more parathyroid glands. Surgical treatment of SPHPT is based on the identification and removal of all abnormal hypersecreting parathyroid glands while preserving normally functioning glands in situ that maintain calcium homeostasis. Conventional parathyroidectomy requires BNE that involves the identification of usually four parathyroid glands, and based on surgeon's judgment and experience, excision of all grossly enlarged glands based on size, weight, color and/or histopathology by frozen section is performed while all normal-sized parathyroid glands are left in situ [3419]. However, this conventional surgical approach can be problematic since these qualitative assessments do not always correlate directly to parathyroid gland secretory function [2021]. If any hypersecreting gland(s) is left behind, hypercalcemia will persist, resulting in a failed operation. Conversely, if all normally functioning parathyroid glands are excised or their blood supply compromised during extensive neck dissection, postoperative hypocalcemia and tetany may occur. This operative approach yields success rates of 97% to 99% when performed by experienced parathyroid surgeons. These curative rates may fall to 70%, however, when traditional parathyroidectomy is performed by inexperienced surgeons [3419].
- Focused parathyroidectomy guided by IPM for SPHPT incorporates the common principles of minimally invasive surgery that result in less dissection, decreased operative time and less morbidity [56789]. IPM allows for the quantitative recognition of parathyroid gland hyperfunction based on PTH secretion during parathyroidectomy and underscores the recognition and understanding of SPHPT as a disease of function rather than form, in which the surgeon is better equipped to treat such patients with quantitative instead of qualitative information for optimal long-term operative success. This paradigm shift of surgical treatment from traditional BNE to focused parathyroidectomy using the intraoperative PTH assay for SPHPT over the last few decades has a comparable reported operative success ranging from 97% to 99% [56789]. Generally, focused parathyroidectomy is performed in patients with a single hyperactive parathyroid gland localized by preoperative MIBI and/or ultrasound studies through a central or lateral incision measuring from 2 to 4 cm. When the abnormal parathyroid gland(s) has been identified and excised, the intraoperative PTH assay is used to confirm that no additional hypersecreting parathyroid tissue remains. When intraoperative PTH levels decrease by >50%, the limited operation is completed [22]. Performed under general or local anesthesia, focused parathyroidectomy guided by IPM can be offered to most patients in the ambulatory setting.
PARADIGM SHIFT OF OPERATIVE APPROACH TO FUNCTION
- SPHPT usually results from an overproduction of PTH by one hyperfunctioning parathyroid gland that usually leads to hypercalcemia. Patients typically have four parathyroid glands (84%), but may have more (supernumerary) glands (13%) or as few as three parathyroid glands (3%) [23]. The incidence of SPHPT increases with age, and ranges from 0.1% to 0.3% [24]. SPHPT occurs more frequently in women than in men with a ratio of 3:1. A parathyroid adenoma is a benign encapsulated tumor that accounts for most cases (85% to 96%) of SPHPT. Although most have single gland disease (SGD), 2% to 5% of patients may have more than one affected parathyroid gland or MGD. MGD or parathyroid hyperplasia is caused by an increase of parenchymal mass within all parathyroid glands, and occurs in 4% to 15% of patients. The incidence of MGD increases in patients with multiple endocrine neoplasia (MEN) types 1 and 2, and non-MEN familial isolated hyperparathyroidism. MGD is treated by either subtotal parathyroidectomy (three and a half glands removed) or total parathyroidectomy with autotransplantation. For patients with MEN, cervical thymectomy should also be performed for supernumerary parathyroid glands. Parathyroid carcinoma is an indolent malignant tumor found in less than 5% of patients.
- The clinical presentation of SPHPT has evolved throughout the years. The classic pentad of kidney “stones,” painful “bones,” abdominal “groans,” lethargic “moans,” and psychic “overtones” are still occasionally seen and described, although most patients present rarely now with these aforementioned dramatic symptoms [2526]. Historically described clinical manifestations of this calcium disorder such as osteitis fibrosa cystica (brown tumors), peptic ulcer disease and pancreatitis among others are now infrequently encountered in developed countries. With the widespread use of serum channel autoanalyzers since the late 1960's, patients with SPHPT most commonly present with abnormal biochemical values before any manifestation of clinical symptoms. At an early stage of diagnosis, most patients with SPHPT are asymptomatic (75% to 80%) with the disease being evident only as hypercalcemia on routine blood tests [2728].
CLINICAL MANIFESTATIONS OF SPHPT
- IPM guided parathyroidectomy should be considered in a patient with a secure biochemical diagnosis of SPHPT as shown by: (1) persistent hypercalcemia, (2) elevated PTH levels, (3) normal renal function, and (4) normal or elevated urinary calcium. When patients have symptoms associated with hypercalcemia or no apparent symptoms that fulfill guidelines as detailed by the Summary Statement from the Fourth International Workshop on the Management of Asymptomatic Primary Hyperparathyroidism, a preoperative localization study can be obtained in an attempt to localize the hyperfunctioning parathyroid gland in the neck for focused parathyroidectomy (Table 1) [29]. Localizing imaging studies, however, should not be used to make the diagnosis of SPHPT or to determine the need for parathyroidectomy. Such imaging studies are used only for guidance of a focused neck or mediastinal exploration when positive. Nonetheless, even when preoperative imaging studies are negative or non-localizing, parathyroidectomy guided by IPM can be performed in patients with described surgical indications.
- IPM has been shown to be useful and predictive of operative success in patients with SPHPT whereas its routine utilization in patients with secondary and tertiary hyperparathyroidism, MEN syndrome, parathyroid cancer and more recent forms of normocalcemic and normohormonal hyperparathyroidism remains unclear [3031323334]. IPM has been used to guide parathyroidectomy for isolated familial hyperparathyroidism with benefits of limited neck operations and lower rates of postoperative hypoparathyroidism, but at lower accuracy associated with higher rates of operative failure and recurrence rates [35]. The information and guidelines for IPM use described in this review article, therefore, are relevant only to the surgical treatment of patients with SPHPT.
INDICATIONS FOR IPM GUIDED PARATHYROIDECTOMY
- Along with confirming the complete excision of all hyperfunctioning parathyroid glands, IPM can also detect the incomplete removal of abnormal parathyroid tissue during the operation, thereby indicating the need for further neck exploration. At the University of Miami, IPM is used to: (1) confirm the complete excision of all hyperfunctioning parathyroid tissue before the operation is finished; (2) guide the surgeon to identify additional hyperfunctioning parathyroid tissue that may necessitate further extensive neck exploration when the intraoperative PTH levels do not drop sufficiently; (3) differentiate parathyroid from non-parathyroid tissues biopsied using measurement of intraoperative PTH levels in fine needle aspiration (FNA) samples; (4) lateralize the side of the neck harboring the hypersecreting parathyroid(s) through differential jugular venous sampling when preoperative localization studies are equivocal; and (5) safely allow limited parathyroidectomy with resection of only hypersecreting gland(s) along with preservation of the normally functioning parathyroid glands in patients with SPHPT.
- During IPM guided parathyroidectomy, PTH hypersecretion by abnormal parathyroid gland(s) is measured by a non-radioactive 2-site immunochemiluminescent antibody that captures and quantifies the unknown amount of hormone in a blood sample. Rapid results are needed for intraoperative PTH dynamics to guide parathyroidectomy, and therefore, point-of-care capability with PTH assay equipment placed in, or in close vicinity to, the operating room is essential. Most intraoperative PTH assays can provide results within an average of 8 to 20 minutes, and correlate well with standard diagnostic assays.
- Several intraoperative PTH drop criteria to predict postoperative eucalcemia and operative success following parathyroidectomy have been published [223637]. However, the first described criterion used to predict postoperative eucalcemia in patients with SPHPT is the “Miami criterion” defined as a >50% PTH decrease from either the highest pre-incision or pre-excision hormone level in a peripheral blood sample obtained 10 minutes after complete excision of all hyperfunctioning parathyroid tissue [1516171822]. This protocol was initially developed and refined at the University of Miami by George L. Irvin III, M.D. Peripheral venous or arterial access for blood collection at specific times during parathyroidectomy is required. During the operation, at least 4 mL of whole blood in a tube with ethylenediaminetetraacetic acid is collected at specific times: (1) a “pre-incision” level prior to skin incision; (2) a “pre-excision” level collected after dissection and just before clamping the abnormal gland's blood supply; (3) a 5-minute level; and (4) 10-minute level after excision of the abnormal parathyroid gland. When peripheral PTH values drop more than 50% from the highest either pre-incision or pre-excision level 10 minutes after the excision of all abnormal parathyroid gland(s), this criterion predicts normal or low calcium levels postoperatively with an overall accuracy of 98% [22]. After this >50% intraoperative PTH decrease occurs, the observed hormone dynamic guides termination of the operation without further exploration or identification of the remaining normally secreting parathyroid glands. If the 10-minute sample does not meet criterion, a delayed sample at 20 minutes is measured and/or further neck exploration is continued until all hypersecreting parathyroid glands are removed confirmed by another >50% decrease from the highest subsequent pre-excision sample [3839].
- In predicting postoperative serum calcium levels, using the Miami criterion during parathyroidectomy guided by IPM has a sensitivity of 98%, specificity of 97%, positive predictive value of 99%, negative predictive value of 90%, and overall accuracy of 97%. Analyzing only those patients with more than 6 months of follow-up including all known operative failures, the sensitivity, specificity, and accuracy remain unchanged [22].
IPM AND THE “MIAMI CRITERION”
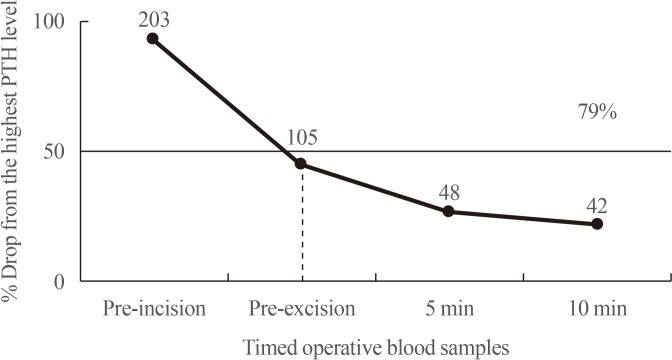
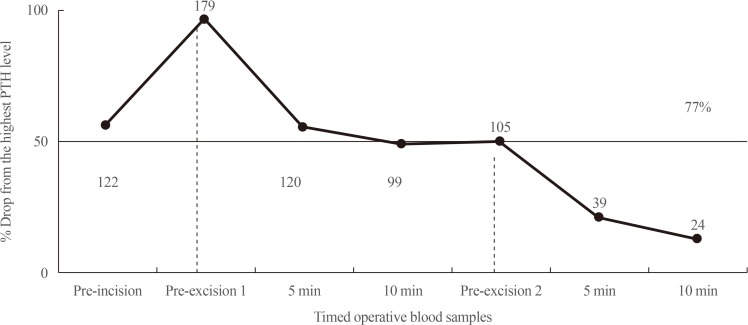
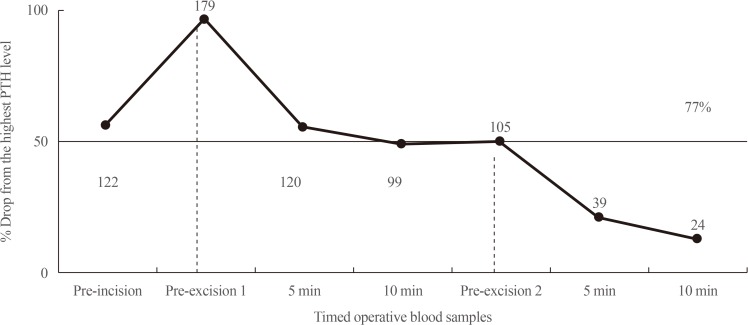
- Understanding the subtleties of intraoperative PTH dynamics allows the surgeon to confidently predict operative success, avoid failure in cases of unsuspected or missed MGD and minimize neck exploration in most patients with SPHPT. IPM provides PTH levels at specific times during the operation, and therefore, the timing of sample collection and interpretation of changes in the hormone values is necessary to ensure a high rate of success. IPM, as used in a patient after excision of a single hypersecreting gland is shown in Fig. 1. With an adequate >50% intraoperative PTH decrease at the 10-minute post-excision interval from the highest pre-incision or pre-excision PTH level, this hormone dynamic predicts postoperative eucalcemia without further exploration of the remaining parathyroid glands in situ. IPM also confirms to the operating surgeon that all underlying hypersecreting parathyroid glands have been excised. Conversely, if PTH levels fail to drop at the 10-minute interval following excision of a suspected hyperfunctioning parathyroid gland, IPM signals that more hypersecreting tissue exists and continued neck exploration with the above described protocol is applied to each additionally removed gland [38]. Another example shows IPM dynamics in a patient with MGD in Fig. 2.
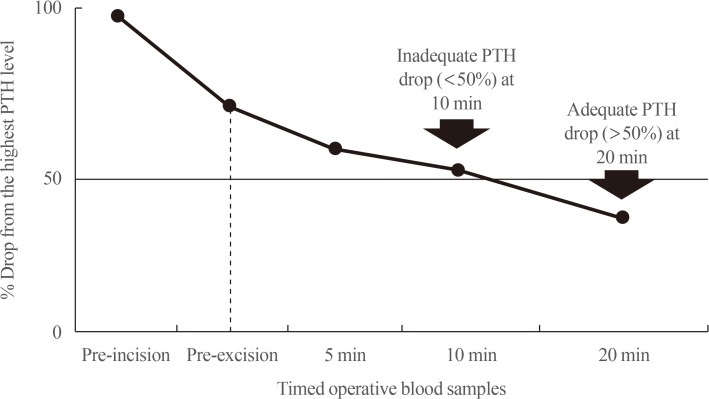
- In some patients, an additional 20-minute PTH level may be obtained if the criterion is not met at 10 minutes after parathyroid gland excision or if the decline dynamics are equivocal (e.g., borderline drop at 50%). In the majority of these patients, the “>50% PTH drop” criterion is achieved with an additional 20-minute measurement that excludes a false negative result and accurately predicts postoperative success (Fig. 3). In 46% of patients with equivocal PTH levels at 10 minutes after parathyroidectomy, a further 20-minute blood sample revealing a >50% PTH decrease has been shown to prevent unnecessary BNE [39]. Ultimately, the surgeon should rely on his/her best judgment to continue neck exploration.
- There are several factors that may adversely influence the accuracy and utility of intraoperative PTH assays in the surgical management of patients with SPHPT. When peripheral intravenous access is obtained before neck exploration, saline infusion maintains this intravenous access patent throughout the operation. Nevertheless, it is prudent to discard 10 cc of blood with saline to avoid blood sample dilution that may lead to falsely decreased PTH measurements. Blood sample hemolysis has also been described to cause falsely low PTH levels, and should not be used [40]. Although shown to increase intraoperative PTH levels, propofol infusions do not significantly influence PTH dynamics [41].
- Although easier to access during parathyroidectomy, jugular venous (central) sampling for blood specimens usually results in higher overall absolute PTH values when compared to peripheral vein samples [4243]. Such PTH levels obtained centrally may take longer to decrease leading to unnecessary neck explorations when a stricter criterion to normal range at 10 minutes is used to meet operative success or prolong the operation for an appropriate PTH decrease [4243]. Although higher PTH levels are measured from central venous specimens, the accuracy of intraoperative PTH dynamics overall are not affected by sample site. Nevertheless, to avoid inaccuracies in the interpretation of IPM dynamics, blood samples during parathyroidectomy should be consistent and obtained from the same site.
- Careful tissue dissection and parathyroid gland excision during the operation is also paramount. To avoid missing a peak PTH level due to manipulation of the offending parathyroid gland during the operation, a “pre-excision” blood sample collected just before ligation of the gland's blood supply should be obtained [224445]. The collection of a “pre-excision” sample may mitigate gland manipulation by the surgeon and a falsely inadequate PTH drop. Conversely, avoiding manipulation of the remaining parathyroid glands will minimize false elevation of intraoperative PTH levels and a delay of its decrease.
INTRAOPERATIVE PTH DYNAMICS
- Although surgeon judgment and experience are important in determining the excision of abnormal parathyroid glands initially, quantitative intraoperative PTH measurement nevertheless can supersede qualitative or subjective evaluation of abnormal parathyroid glands based on observed gland size, color, weight and/or histopathology by frozen section. MIBI scintigraphy and high-resolution neck ultrasonography, in contrast, play an important role in focused operations by identifying the anatomical location of an abnormal hypersecreting and/or enlarged gland, and when localized preoperatively, allow for minimal dissection of the targeted area and excision of this diseased parathyroid gland. However, in patients where imaging studies fail to correctly identify the offending parathyroid gland or in those patients with MGD, IPM can determine if all hypersecreting tissue has been removed or if the need for further exploration of more underlying abnormal parathyroid glands. When small incisions are used, and other parathyroid glands are not routinely visualized, IPM provides assurance to the surgeon during the operation that all hypersecreting parathyroid tissue has been excised.
- IPM guided parathyroidectomy and BNE
- Studies demonstrate that operative success and complication rates for IPM guided parathyroidectomy are comparable to conventional BNE [56789]. In one study of 656 consecutive patients over 11 years where 255 underwent focused parathyroidectomy with IPM and 401 conventional BNE, the cure rates were 99% and 97% with complication rates of 1.2% and 3%, respectively. Parathyroidectomy guided by IPM also had a reduced operating time (1.3 hours vs. 2.4 hours), and a reduction in length of hospitalization (0.24 days vs. 1.64 days) when compared to BNE [5]. In another subsequent study of 718 patients over 34 years, the cure rates for focused parathyroidectomy guided by IPM and BNE were 97% and 94%, respectively [7]. In a 5-year follow-up of a randomized controlled trial, focused parathyroidectomy guided by IPM provided the same long-term results as traditional BNE in patients with primary hyperparathyroidism [46]. In a multicenter study of patients with primary hyperparathyroidism, despite inaccuracy of localization studies as well as a large number of patients undergoing BNE, IPM decreased postoperative rates of hypocalcemia and increased early operative success rates [47].
- Parathyroidectomy guided by IPM compared to conventional BNE results in fewer complications, less neck dissection, shorter operative times, smaller incisions, increased use of local anesthesia, and emphasis on outpatient procedures [5678948]. IPM has been shown to be cost effective in the United States mainly because it allows for ambulatory or outpatient parathyroidectomy [4849]. Focused parathyroidectomy with IPM allows for approximately a 50% decrease in hospital costs and patient charges when compared to conventional BNE [49].
- IPM and equivocal/discordant or negative localization studies
- When localization studies are equivocal, discordant or negative in close to 40% of patients, IPM is invaluable in achieving operative success [50]. MIBI scans can be completely negative, have a single wrong focus, show multiple foci both correct and incorrect, and miss multiple gland involvement [50]. IPM used as an adjunct to parathyroidectomy can prevent failure when localization studies are incorrect, which is not always evident until in the operating room or at completion of the operation [51]. Preoperative MIBI and neck ultrasound have been shown to be concordant only 50% to 60% of the time, thereby leaving a great number of patients with no definitive or discordant localization. Discordance between MIBI and ultrasound has been reported to be as high as 38% in consecutive patients treated by parathyroidectomy with an 11% rate of MGD [50]. When preoperative localization studies are concordant for SGD, the use of IPM may have marginal value [375052]. However, in such instances where there are discordant studies, IPM has been shown to be of significant value in minimizing missed abnormal parathyroid glands.
- In patients with SPHPT undergoing initial parathyroidectomy and negative preoperative MIBI and ultrasound imaging, there is an increased risk for unsuccessful BNE, operative failure and missed MGD [51]. In a prospective multicenter study of 984 patients subjected to preoperative localization with MIBI scinitigraphy and neck ultrasound who underwent initial parathyroidectomy, there were 173 patients who had both imaging studies negative [53]. Of this group with negative localization studies, in a subset of 83 patients who had IPM used during their parathyroid operations compared to 90 patients who did not, the risk for persistent hyperparathyroidism decreased from 26% to 8% and the risk of postoperative hypocalcemia from 16% to 8% at 6 weeks follow-up. As supported by the aforementioned studies, the routine use of IPM in patients with negative or discordant localization studies has been recommended in a position statement by the European Society of Endocrine Surgeons [52]. Similarly, the use of IPM is recommended for patients with SPHPT undergoing focused parathyroidectomy on the basis of a single preoperative localizing imaging study.
- IPM and MGD
- The reported MGD rates of 3% to 5% using the Miami or “>50% intraoperative PTH drop” criterion are significantly lower than rates reported for stricter intraoperative PTH criteria or BNE (15% to 30%) [1011545556]. This has led to the belief that this >50% PTH decrease during parathyroidectomy misses MGD leading to unacceptable operative failure rates as high as 16% [57]. Other series of parathyroidectomy guided by this intraoperative >50% PTH decrease criterion report operative success rates of 96% to 98%, and fail to show these hypothetical high failure rates [56789]. In a study of 103 patients who underwent initial parathyroidectomy for SPHPT, the operative success rate was 96% with the use of IPM [58]. Although MIBI localization was unreliable in demonstrating MGD in this patient series, IPM was shown to differentiate between single and multiple gland disease to ensure long term operative success. In this study, IPM correctly predicted all patients with MGD [58]. At the authors' institution, operative success was 98% in 164 treated patients with a 2% failure rate. Recurrence rate at 10 years after undergoing focused parathyroidectomy guided by IPM was 3%. This long-term study indicates that there may be an overestimation of the predicted incidence for MGD; if such higher rates of missed MGD were correct, a 16% or greater recurrence rate would have been appreciated [11].
- When stricter >50% PTH decrease criteria to normal range are used or conventional BNE is performed after the “>50% PTH drop” has occurred, additional enlarged, but normally functioning glands may be found as previously described [1157]. Nevertheless, proponents of BNE continue to base the success of their operations on the ability to differentiate between normal and abnormal glands based on qualitative or subjective criteria that includes size alone, weight, color and/or histopathology by frozen section [57]. Since operative success without the excision of these additionally found “enlarged” glands has been reportedly shown to remain the same, the answer to this dilemma may rest in that grossly enlarged glands may not always be hyperfunctioning [71159]. Prior reports have indicated that parathyroid gland size and histology does not always correlate with parathyroid function [2021].
- In a prospective randomized study of patients that underwent parathyroidectomy determined by gland size during BNE, there was a higher incidence (10%) of MGD compared to patients who underwent parathyroidectomy determined by gland function with IPM (3%). Despite fewer glands excised in the IPM group, the operative success for both groups was similar [7]. The same findings were reported in another study where there was a higher incidence of MGD in patients who underwent BNE (16.5%) compared to those patients who underwent parathyroidectomy guided by IPM (11.1%) despite similar surgical success rates [59]. These aforementioned findings and other mounting evidence suggest that the routine excision of parathyroid glands based on size, weight, color and/or histopathology by frozen section in an effort to minimize missed MGD, and thus operative failure, may actually lead to the unfortunate removal of various sized, but normally functioning, parathyroid glands not contributing to SPHPT [11].
- IPM and stricter criteria
- Over the last few years, the “>50% intraoperative PTH drop” criterion has been modified by some with the ultimate goal of minimizing missed MGD, operative failure and improving cost-effectiveness [223637]. Stricter criteria that have been proposed include a larger PTH level percent drop (>65% to 70%) and/or return of the final PTH to within normal range, or a PTH decrease at 5 minutes after gland excision [363756]. There is some evidence to suggest that modification of the original and least strict intraoperative >50% PTH decrease criterion to stricter requirements may slightly decrease the number of operative failures, but will significantly increase the incidence of false negative results leading to unnecessary further neck explorations and lowering its overall accuracy.
- Studies have shown that the Miami criterion followed by the Vienna criterion are the most balanced among all criteria published in the literature, with the highest accuracy in the intraoperative prediction of operative success (Table 2) [223637]. Conversely, the Rome criterion followed by the Halle criterion, may be useful in the intraoperative detection of underlying MGD. However, the application of these stricter criteria in patients with SPHPT and concordant preoperative imaging studies during initial parathyroidectomy would result in a significantly higher number of unnecessary BNE with a marginal improvement in operative success [223637]. Even so, almost all patients with an intraoperative >50% PTH decrease, without regard for the absolute PTH level at the conclusion of the operation, still continue to be eucalcemic after parathyroidectomy without a significant increased incidence of operative failure [60]. Nevertheless, operating surgeons should validate their IPM criterion to maximize operative success and minimize excessive neck exploration at their respective institutions.
APPLICATIONS OF IPM GUIDED PARATHYROIDECTOMY
- Since 1993, parathyroid surgeries have been guided exclusively by intraoperative PTH dynamics at the University of Miami. Conventional BNE is no longer performed as the initial approach unless there are negative or equivocal preoperative localizing studies confirmed by IPM. All patients have total serum calcium levels measured within one or 2 days postoperatively, followed by measurements of total serum calcium and PTH levels at 2, 6 months, and yearly thereafter. At the author's institution, operative success is considered when a patient has normal or low calcium levels for at least 6 months after parathyroidectomy. Operative failure is defined as persistent hypercalcemia and elevated intact PTH levels occurring within 6 months of parathyroidectomy. Recurrent disease is defined as hypercalcemia and high intact PTH levels occurring later than 6 months following successful parathyroidectomy. MGD is considered the presence of two or more hyperfunctioning glands at the time of parathyroidectomy as demonstrated by IPM or when removal of one gland results in operative failure.
- In a series of 173 consecutive patients with SPHPT underwent IPM guided parathyroidectomy at the University of Miami, 164 patients had more than 6 months of follow-up with a mean postoperative follow-up of 83 months (range, 6 to 180) [11]. Overall, 98% of these 164 consecutive patients had successful parathyroid surgery and 2% were operative failures. There were five patients (3%) who developed recurrent disease later at 2, 4, 9, 10, and 12 years after their initial parathyroidectomy. SGD was found in 96% of patients, and MGD was found in 4% of patients. Using the Miami criterion, IPM correctly predicted postoperative success in 98% of patients at 6 months. IPM predicted the presence of MGD in six of seven patients. Of this group, there was a subset of 44 patients with a mean follow-up of 142 months (range, 120 to 180) after IPM guided parathyroidectomy who did not develop recurrent disease [11]. Of these patients, 43 had SGD and one had MGD identified by IPM at the time of operation. All 44 patients have remained eucalcemic almost 12 years after surgical resection. Such postoperative outcomes indicate IPM guided parathyroidectomy allows for limited dissection of SGD in patients with SPHPT with durable long-term eucalcemia.
- In a later study from another institution of 1,368 patients who underwent unilateral or BNEs with IPM for primary hyperparathyroidism, there were no statistical differences in disease recurrence between groups (2.5% vs. 2.1%, P=0.68) with a median follow-up of 9.2 months [61]. However, intraoperative PTH percentage decrease was protective against disease for the entire and unilateral neck exploration group. Furthermore, higher postoperative PTH levels also independently predicted disease recurrence. Although either operative approach did not independently predict recurrent hyperparathyroidism, intraoperative PTH percentage decrease was another factor to help determine need for conversion to BNE and help guide follow-up after successful parathyroidectomy [61].
- In yet another study of 1,108 patients who underwent initial parathyroidectomy using IPM for SPHPT with a mean follow-up of 21.6 months (range, 6 to 171.6), a final intraoperative PTH value that dropped >50% from baseline to within normal range was highly predictive of (98.5%) operative success [62]. Additionally, disease recurrence was more likely in patients with a final intraoperative PTH value between 41 to 65 pg/mL (1.1%) than those patients with a final value of <40 pg/mL (0%). Such findings suggest that IPM facilitates a high rate of initial operative success for SPHPT, and that patients with a final intraoperative PTH value >40 pg/mL despite a >50% decrease should be continually monitored beyond 6 months for long-term disease recurrence [62].
- Such postoperative outcomes indicate IPM guided parathyroidectomy allows for limited dissection of SGD in patients with SPHPT with predictive operative success at 6 months, low recurrence rates and durable long-term eucalcemia. Nevertheless, as these aforementioned studies demonstrate, the accuracy of IPM is highly dependent on the criteria and its implementation in predicting successful parathyroidectomy.
LONG TERM RESULTS OF IPM GUIDED PARATHYROIDECTOMY
- The intraoperative PTH assay used with the aforementioned criterion not only determines the complete resection of all hypersecreting parathyroid tissue, but can also help the surgeon lateralize and identify the offending parathyroid gland(s) in patients with negative or equivocal preoperative imaging studies. Additionally, the intraoperative PTH assay can be used to help lateralize the abnormal hyperfunctioning parathyroid gland in patients undergoing reoperative parathyroidectomy, and to predict operative success as well as obviate the need for further extensive exploration in a previously surgically scarred neck.
- Differential internal jugular venous sampling
- When conventional BNE for patients with negative preoperative localization studies is performed, differential jugular venous sampling can be used in these patients to lateralize the side of the neck harboring the hyperfunctioning parathyroid gland [636465]. When in the operating room, blood samples from the most inferior portion of each internal jugular vein, preferably guided by ultrasound, are taken for rapid PTH measurement before skin incision. This technique that is positive in 70% to 80% of cases can lateralize to the side of the neck containing the highest PTH level (10% higher than the opposite side) leading to successful unilateral neck exploration when used in conjunction with IPM [6364].
- Biochemical fine needle aspiration
- FNA of tissue for PTH measurement can differentiate parathyroid glands from other anatomic structures of the neck with 100% specificity. A 25-gauge needle attached to a syringe is used to aspirate the structure suspicious for parathyroid tissue. The content aspirated in the needle is diluted with 1 cc of saline solution, centrifuged, and the supernatant is used for PTH measurement with the rapid intraoperative assay [66]. This technique provides prompt tissue identification without frozen section, and it can be helpful when parathyroid gland localization is challenging, especially when an intrathyroidal parathyroid gland, indeterminate exophytic thyroid nodule, or enlarged lymph nodes are present.
ADDITIONAL USES FOR THE INTRAOPERATIVE PTH ASSAY
- Focused parathyroidectomy guided IPM has been shown to be effective in assuring operative success through minimal dissection and selected parathyroid gland excision. Using the Miami or “>50% intraoperative PTH drop” criterion, only the hyperfunctioning parathyroid gland(s) is excised without visualizing or disturbing the remaining normally functioning parathyroid glands in situ. Instead of the traditional means of identifying abnormal parathyroid glands based on size, weight and/or histopathology, IPM allows for a precise quantitative recognition of parathyroid gland hyperfunction based on PTH secretion during parathyroidectomy. The use of IPM underscores the recognition and understanding of SPHPT as a disease of function rather than form, where the surgeon is better equipped to treat such patients with quantitative instead of qualitative information for durable long-term operative success. There has been a significant paradigm shift of treatment from conventional to focused parathyroidectomy with IPM for SPHPT over the last few decades. Guided by intraoperative PTH levels, parathyroidectomy has evolved into a safe, most successful and rapid operation, requiring minimal dissection and can be performed in an ambulatory setting.
CONCLUSIONS
-
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
Article information
- 1. Mandl F. Klinisches und experimentelles zur frage der lokalisierten und generalisierten ostitis fibrosa: unter besonderer berücksichtigung der therapie der letzteren. Teil 2. Arch Klin Chir 1926;143:245–248.
- 2. Niederle BE, Schmidt G, Organ CH, Niederle B. Albert J and his surgeon: a historical reevaluation of the first parathyroidectomy. J Am Coll Surg 2006;202:181–190. ArticlePubMed
- 3. van Heerden JA, Grant CS. Surgical treatment of primary hyperparathyroidism: an institutional perspective. World J Surg 1991;15:688–692. ArticlePubMedPDF
- 4. Allendorf J, DiGorgi M, Spanknebel K, Inabnet W, Chabot J, Logerfo P. 1112 Consecutive bilateral neck explorations for primary hyperparathyroidism. World J Surg 2007;31:2075–2080. ArticlePubMedPDF
- 5. Udelsman R. Six hundred fifty-six consecutive explorations for primary hyperparathyroidism. Ann Surg 2002;235:665–670. ArticlePubMedPMC
- 6. Westerdahl J, Lindblom P, Bergenfelz A. Measurement of intraoperative parathyroid hormone predicts long-term operative success. Arch Surg 2002;137:186–190. ArticlePubMed
- 7. Irvin GL 3rd, Carneiro DM, Solorzano CC. Progress in the operative management of sporadic primary hyperparathyroidism over 34 years. Ann Surg 2004;239:704–708. ArticlePubMedPMC
- 8. Chen H, Pruhs Z, Starling JR, Mack E. Intraoperative parathyroid hormone testing improves cure rates in patients undergoing minimally invasive parathyroidectomy. Surgery 2005;138:583–587. ArticlePubMed
- 9. Grant CS, Thompson G, Farley D, van Heerden J. Primary hyperparathyroidism surgical management since the introduction of minimally invasive parathyroidectomy: Mayo Clinic experience. Arch Surg 2005;140:472–478. ArticlePubMed
- 10. Molinari AS, Irvin GL 3rd, Deriso GT, Bott L. Incidence of multiglandular disease in primary hyperparathyroidism determined by parathyroid hormone secretion. Surgery 1996;120:934–936. ArticlePubMed
- 11. Lew JI, Irvin GL 3rd. Focused parathyroidectomy guided by intra-operative parathormone monitoring does not miss multiglandular disease in patients with sporadic primary hyperparathyroidism: a 10-year outcome. Surgery 2009;146:1021–1027. ArticlePubMed
- 12. Sackett WR, Barraclough B, Reeve TS, Delbridge LW. Worldwide trends in the surgical treatment of primary hyperparathyroidism in the era of minimally invasive parathyroidectomy. Arch Surg 2002;137:1055–1059. ArticlePubMed
- 13. Greene AB, Butler RS, McIntyre S, Barbosa GF, Mitchell J, Berber E, et al. National trends in parathyroid surgery from 1998 to 2008: a decade of change. J Am Coll Surg 2009;209:332–343. ArticlePubMed
- 14. Nussbaum SR, Zahradnik RJ, Lavigne JR, Brennan GL, Nozawa-Ung K, Kim LY, et al. Highly sensitive two-site immunoradiometric assay of parathyrin, and its clinical utility in evaluating patients with hypercalcemia. Clin Chem 1987;33:1364–1367. ArticlePubMedPDF
- 15. Irvin GL 3rd, Dembrow VD, Prudhomme DL. Operative monitoring of parathyroid gland hyperfunction. Am J Surg 1991;162:299–302. ArticlePubMed
- 16. Irvin GL 3rd, Deriso GT 3rd. A new, practical intraoperative parathyroid hormone assay. Am J Surg 1994;168:466–468. ArticlePubMed
- 17. Irvin GL 3rd, Prudhomme DL, Deriso GT, Sfakianakis G, Chandarlapaty SK. A new approach to parathyroidectomy. Ann Surg 1994;219:574–579. ArticlePubMedPMC
- 18. Irvin GL 3rd, Sfakianakis G, Yeung L, Deriso GT, Fishman LM, Molinari AS, et al. Ambulatory parathyroidectomy for primary hyperparathyroidism. Arch Surg 1996;131:1074–1078. ArticlePubMed
- 19. Kaplan EL, Yashiro T, Salti G. Primary hyperparathyroidism in the 1990s. Choice of surgical procedures for this disease. Ann Surg 1992;215:300–317. ArticlePubMedPMC
- 20. Mun HC, Conigrave A, Wilkinson M, Delbridge L. Surgery for hyperparathyroidism: does morphology or function matter most? Surgery 2005;138:1111–1120. ArticlePubMed
- 21. Elliott DD, Monroe DP, Perrier ND. Parathyroid histopathology: is it of any value today? J Am Coll Surg 2006;203:758–765. ArticlePubMed
- 22. Carneiro DM, Solorzano CC, Nader MC, Ramirez M, Irvin GL 3rd. Comparison of intraoperative iPTH assay (QPTH) criteria in guiding parathyroidectomy: which criterion is the most accurate. Surgery 2003;134:973–979. ArticlePubMed
- 23. Akerstrom G, Malmaeus J, Bergstrom R. Surgical anatomy of human parathyroid glands. Surgery 1984;95:14–21. PubMed
- 24. Uden P, Chan A, Duh QY, Siperstein A, Clark OH. Primary hyperparathyroidism in younger and older patients: symptoms and outcome of surgery. World J Surg 1992;16:791–797. ArticlePubMedPDF
- 25. St Goar WT. Gastrointestinal symptoms as a clue to the diagnosis of primary hyperparathyroidism: a review of 45 cases. Ann Intern Med 1957;46:102–118. ArticlePubMed
- 26. Chan AK, Duh QY, Katz MH, Siperstein AE, Clark OH. Clinical manifestations of primary hyperparathyroidism before and after parathyroidectomy. A case-control study. Ann Surg 1995;222:402–412. ArticlePubMedPMC
- 27. Bilezikian JP, Potts JT Jr. Asymptomatic primary hyperparathyroidism: new issues and new questions: bridging the past with the future. J Bone Miner Res 2002;17:N57–N67. PubMed
- 28. Eigelberger MS, Cheah WK, Ituarte PH, Streja L, Duh QY, Clark OH. The NIH criteria for parathyroidectomy in asymptomatic primary hyperparathyroidism: are they too limited. Ann Surg 2004;239:528–535. ArticlePubMedPMC
- 29. Bilezikian JP, Brandi ML, Eastell R, Silverberg SJ, Udelsman R, Marcocci C, et al. Guidelines for the management of asymptomatic primary hyperparathyroidism: summary statement from the Fourth International Workshop. J Clin Endocrinol Metab 2014;99:3561–3569. ArticlePubMedPMC
- 30. Tonelli F, Spini S, Tommasi M, Gabbrielli G, Amorosi A, Brocchi A, et al. Intraoperative parathormone measurement in patients with multiple endocrine neoplasia type I syndrome and hyperparathyroidism. World J Surg 2000;24:556–562. ArticlePubMedPDF
- 31. Chou FF, Lee CH, Chen JB, Hsu KT, Sheen-Chen SM. Intraoperative parathyroid hormone measurement in patients with secondary hyperparathyroidism. Arch Surg 2002;137:341–344. ArticlePubMed
- 32. Haustein SV, Mack E, Starling JR, Chen H. The role of intraoperative parathyroid hormone testing in patients with tertiary hyperparathyroidism after renal transplantation. Surgery 2005;138:1066–1071. ArticlePubMed
- 33. Solorzano CC, Carneiro-Pla DM, Lew JI, Rodgers SE, Montano R, Irvin GL 3rd. Intra-operative parathyroid hormone monitoring in patients with parathyroid cancer. Ann Surg Oncol 2007;14:3216–3222. ArticlePubMedPDF
- 34. Lim JY, Herman MC, Bubis L, Epelboym I, Allendorf JD, Chabot JA, et al. Differences in single gland and multigland disease are seen in low biochemical profile primary hyperparathyroidism. Surgery 2017;161:70–77. ArticlePubMed
- 35. Carneiro DM, Irvin GL 3rd, Inabnet WB. Limited versus radical parathyroidectomy in familial isolated primary hyperparathyroidism. Surgery 2002;132:1050–1054. ArticlePubMed
- 36. Chiu B, Sturgeon C, Angelos P. Which intraoperative parathyroid hormone assay criterion best predicts operative success? A study of 352 consecutive patients. Arch Surg 2006;141:483–487. ArticlePubMed
- 37. Barczynski M, Konturek A, Hubalewska-Dydejczyk A, Cichon S, Nowak W. Evaluation of Halle, Miami, Rome, and Vienna intraoperative iPTH assay criteria in guiding minimally invasive parathyroidectomy. Langenbecks Arch Surg 2009;394:843–849. ArticlePubMedPDF
- 38. Irvin GL 3rd, Solorzano CC, Carneiro DM. Quick intraoperative parathyroid hormone assay: surgical adjunct to allow limited parathyroidectomy, improve success rate, and predict outcome. World J Surg 2004;28:1287–1292. ArticlePubMedPDF
- 39. Khan ZF, Picado O, Marcadis AR, Farra JC, Lew JI. Additional 20-minute intraoperative parathormone measurement can minimize unnecessary bilateral neck exploration. J Surg Res 2019;235:264–269. ArticlePubMed
- 40. Moalem J, Ruan DT, Farkas RL, Shen WT, Miller S, Duh QY, et al. Prospective evaluation of the rate and impact of hemolysis on intraoperative parathyroid hormone (IOPTH) assay results. Ann Surg Oncol 2010;17:2963–2969. ArticlePubMedPDF
- 41. Sippel RS, Becker YT, Odorico JS, Springman SR, Chen H. Does propofol anesthesia affect intraoperative parathyroid hormone levels? A randomized, prospective trial. Surgery 2004;136:1138–1142. ArticlePubMed
- 42. Woodrum DT, Saunders BD, England BG, Burney RE, Doherty GM, Gauger PG. The influence of sample site on intraoperative PTH monitoring during parathyroidectomy. Surgery 2004;136:1169–1175. ArticlePubMed
- 43. Beyer TD, Chen E, Ata A, DeCresce R, Prinz RA, Solorzano CC. A prospective evaluation of the effect of sample collection site on intraoperative parathormone monitoring during parathyroidectomy. Surgery 2008;144:504–509. ArticlePubMed
- 44. Yang GP, Levine S, Weigel RJ. A spike in parathyroid hormone during neck exploration may cause a false-negative intraoperative assay result. Arch Surg 2001;136:945–949. ArticlePubMed
- 45. Teo R, Farra JC, Khan ZF, Marcadis AR, Lew JI. Intraoperative parathormone spikes during parathyroidectomy may be associated with multiglandular disease. Surgery 2018;163:393–396. ArticlePubMed
- 46. Westerdahl J, Bergenfelz A. Unilateral versus bilateral neck exploration for primary hyperparathyroidism: five-year follow-up of a randomized controlled trial. Ann Surg 2007;246:976–980. ArticlePubMed
- 47. Bergenfelz AO, Jansson SK, Wallin GK, Martensson HG, Rasmussen L, Eriksson HL, et al. Impact of modern techniques on short-term outcome after surgery for primary hyperparathyroidism: a multicenter study comprising 2,708 patients. Langenbecks Arch Surg 2009;394:851–860. ArticlePubMedPDF
- 48. Chen H, Sokoll LJ, Udelsman R. Outpatient minimally invasive parathyroidectomy: a combination of sestamibi-SPECT localization, cervical block anesthesia, and intraoperative parathyroid hormone assay. Surgery 1999;126:1016–1021. ArticlePubMed
- 49. Fahy BN, Bold RJ, Beckett L, Schneider PD. Modern parathyroid surgery: a cost-benefit analysis of localizing strategies. Arch Surg 2002;137:917–922. ArticlePubMed
- 50. Lew JI, Solorzano CC, Montano RE, Carneiro-Pla DM, Irvin GL 3rd. Role of intraoperative parathormone monitoring during parathyroidectomy in patients with discordant localization studies. Surgery 2008;144:299–306. ArticlePubMed
- 51. Lew JI, Rivera M, Irvin GL 3rd, Solorzano CC. Operative failure in the era of focused parathyroidectomy: a contemporary series of 845 patients. Arch Surg 2010;145:628–633. ArticlePubMed
- 52. Bergenfelz AO, Hellman P, Harrison B, Sitges-Serra A, Dralle H. European Society of Endocrine Surgeons. Positional statement of the European Society of Endocrine Surgeons (ESES) on modern techniques in pHPT surgery. Langenbecks Arch Surg 2009;394:761–764. ArticlePubMedPDF
- 53. Bergenfelz AO, Wallin G, Jansson S, Eriksson H, Martensson H, Christiansen P, et al. Results of surgery for sporadic primary hyperparathyroidism in patients with preoperatively negative sestamibi scintigraphy and ultrasound. Langenbecks Arch Surg 2011;396:83–90. ArticlePubMedPDF
- 54. Lee NC, Norton JA. Multiple-gland disease in primary hyperparathyroidism: a function of operative approach? Arch Surg 2002;137:896–899. ArticlePubMed
- 55. Haciyanli M, Lal G, Morita E, Duh QY, Kebebew E, Clark OH. Accuracy of preoperative localization studies and intraoperative parathyroid hormone assay in patients with primary hyperparathyroidism and double adenoma. J Am Coll Surg 2003;197:739–746. ArticlePubMed
- 56. Clerici T, Brandle M, Lange J, Doherty GM, Gauger PG. Impact of intraoperative parathyroid hormone monitoring on the prediction of multiglandular parathyroid disease. World J Surg 2004;28:187–192. ArticlePubMedPDF
- 57. Siperstein A, Berber E, Barbosa GF, Tsinberg M, Greene AB, Mitchell J, et al. Predicting the success of limited exploration for primary hyperparathyroidism using ultrasound, sestamibi, and intraoperative parathyroid hormone: analysis of 1158 cases. Ann Surg 2008;248:420–428. ArticlePubMed
- 58. Westerdahl J, Bergenfelz A. Sestamibi scan-directed parathyroid surgery: potentially high failure rate without measurement of intraoperative parathyroid hormone. World J Surg 2004;28:1132–1138. ArticlePubMedPDF
- 59. McGill J, Sturgeon C, Kaplan SP, Chiu B, Kaplan EL, Angelos P. How does the operative strategy for primary hyperparathyroidism impact the findings and cure rate? A comparison of 800 parathyroidectomies. J Am Coll Surg 2008;207:246–249. ArticlePubMed
- 60. Carneiro-Pla DM, Solorzano CC, Lew JI, Irvin GL 3rd. Long-term outcome of patients with intraoperative parathyroid level remaining above the normal range during parathyroidectomy. Surgery 2008;144:989–993. ArticlePubMed
- 61. Schneider DF, Mazeh H, Chen H, Sippel RS. Predictors of recurrence in primary hyperparathyroidism: an analysis of 1386 cases. Ann Surg 2014;259:563–568. ArticlePubMedPMC
- 62. Wharry LI, Yip L, Armstrong MJ, Virji MA, Stang MT, Carty SE, et al. The final intraoperative parathyroid hormone level: how low should it go? World J Surg 2014;38:558–563. ArticlePubMedPDF
- 63. Taylor J, Fraser W, Banaszkiewicz P, Drury P, Atkins P. Lateralization of parathyroid adenomas by intra-operative parathormone estimation. J R Coll Surg Edinb 1996;41:174–177. PubMed
- 64. Udelsman R, Osterman F, Sokoll LJ, Drew H, Levine MA, Chan DW. Rapid parathyroid hormone measurement during venous localization. Clin Chim Acta 2000;295:193–198. ArticlePubMed
- 65. Ito F, Sippel R, Lederman J, Chen H. The utility of intraoperative bilateral internal jugular venous sampling with rapid parathyroid hormone testing. Ann Surg 2007;245:959–963. ArticlePubMedPMC
- 66. Perrier ND, Ituarte P, Kikuchi S, Siperstein AE, Duh QY, Clark OH, et al. Intraoperative parathyroid aspiration and parathyroid hormone assay as an alternative to frozen section for tissue identification. World J Surg 2000;24:1319–1322. ArticlePubMedPDF
References
Intraoperative parathyroid hormone (PTH) dynamics after successful excision of a single hyperfunctioning parathyroid gland. With a drop at the 10-minute post-excision interval of 79% from the highest PTH level, this hormone dynamic predicts a postoperative return to eucalcemia and successful parathyroidectomy. Dotted line shows time of gland excision.

Intraoperative parathyroid hormone (PTH) dynamics during successful parathyroidectomy in a patient presenting with multiglandular disease. An intraoperative pre-incision level of 122 pg/mL, excision of an abnormal left inferior parathyroid gland led to a rise of PTH level to 179 pg/mL. After excision of this hypersecreting gland, the PTH assay showed no decrease at 5 minutes (120 pg/mL) and 10 minutes (98 pg/mL). Continued neck exploration revealed another abnormal hypersecreting parathyroid gland. The third and fourth glands appeared grossly normal. The expected hormone level did not decrease significantly until excision of the second hyperfunctioning parathyroid gland. With a 77% decrease in the 10-minute sample (24 pg/mL) compared with the second pre-excision plasma sample (105 pg/mL), no remaining hypersecreting parathyroid tissue was present. Dotted line shows time of gland excision.
Intraoperative parathyroid hormone (PTH) dynamics in a patient where the intraoperative >50% PTH decrease criterion is not met at 10 minutes after parathyroid gland excision or if the decline dynamics are equivocal (e.g., borderline PTH drop at 50%). In the majority of patients, the “>50% intraoperative PTH drop” criterion is achieved with an additional 20-minute PTH measurement that excludes a false negative result, accurately predicts postoperative success and prevents unnecessary bilateral neck exploration. Dotted line shows time of gland excision.
Guidelines from the Fourth International Workshop on the Management of Asymptomatic Primary Hyperparathyroidism [29]
Patients need to meet only one of these criteria to be advised to undergo parathyroidectomy. They do not need to meet more than one these criteria.
BMD, bone mineral density; DXA, dual energy X-ray absorptiometry; CT, computed tomography; MRI, magnetic resonance imaging; VFA, vertebral fracture assessment.
aThe use of Z-scores instead of T-scores is recommended in evaluating BMD in premenopausal women and men younger than 50 years; bMost clinicians will first obtain a 24-hour urine for calcium excretion. If marked hypercalciuria is present (400 mg/day [10 mmol/day]), evidence of calcium-containing stone risk should be sought by a urinary biochemical stone risk profile. The presence of abnormal findings indicating increased calcium-containing stone risk and marked hypercalciuria is a guideline for parathyroidectomy.
Most Common Intraoperative PTH Criteria for Prediction of Operative Success [37]
Figure & Data
References
Citations
- Intraoperative parathyroid hormone monitoring in parathyroidectomy for hyperparathyroidism: a protocol for a network meta-analysis of diagnostic test accuracy
Phillip Staibano, Kevin Um, Sheila Yu, Mohit Bhandari, Michael K. Gupta, Michael Au, JEM (Ted) Young, Han Zhang
Frontiers in Surgery.2024;[Epub] CrossRef - Primary Hyperparathyroidism
Saba Kurtom, Sally E. Carty
Surgical Clinics of North America.2024;[Epub] CrossRef - Parathyroidectomy for primary hyperparathyroidism: A retrospective analysis of localization, surgical characteristics, and treatment outcomes
Dongbin Ahn, Ji Hye Kwak, Gil Joon Lee, Jin Ho Sohn
Asian Journal of Surgery.2023; 46(2): 788. CrossRef - Magnitude of parathyroid hormone elevation in primary hyperparathyroidism: Does time of day matter?
C. Corbin Frye, Janessa Sullivan, Sai Anusha Sanka, Jingxia Liu, L. Michael Brunt, William Gillanders, Taylor C. Brown, T.K. Pandian
Surgery.2023; 173(3): 659. CrossRef - Analysis of intraoperative laboratory measurements and imaging techniques such as Tc-99 m-MIBI SPECT/CT, 18F-fluorocholine PET/CT and ultrasound in patients operated with prediagnosis of parathyroid adenoma
Nurullah Bilen, Mehmet Avni Gokalp, Latif Yilmaz, Alper Aytekin, Ilyas Baskonus
Irish Journal of Medical Science (1971 -).2023; 192(4): 1695. CrossRef - Intraoperative Parathyroid Hormone Monitoring Is of Limited Usefulness in Guiding Autotransplantation in Reoperative or Subtotal Parathyroidectomy for Primary Hyperparathyroidism
Bradley A. Richards, Robert A. Vierkant, Benzon M. Dy, Trenton R. Foster, Travis J. McKenzie, Melanie L. Lyden
The American Surgeon™.2023; 89(12): 5421. CrossRef - Does 18F-Fluorocholine PET/CT add value to positive parathyroid scintigraphy in the presurgical assessment of primary hyperparathyroidism?
Alessio Imperiale, Jacob Bani, Gianluca Bottoni, Adrien Latgé, Céline Heimburger, Ugo Catrambone, Michel Vix, Giorgio Treglia, Arnoldo Piccardo
Frontiers in Medicine.2023;[Epub] CrossRef - Intraoperative Identification of Thyroid and Parathyroid Tissues During Human Endocrine Surgery Using the MasSpec Pen
Rachel J. DeHoog, Mary E. King, Michael F. Keating, Jialing Zhang, Marta Sans, Clara L. Feider, Kyana Y. Garza, Alena Bensussan, Anna Krieger, John Q. Lin, Sunil Badal, Elizabeth Alore, Christopher Pirko, Kirtan Brahmbhatt, Wendong Yu, Raymon Grogan, Livi
JAMA Surgery.2023; 158(10): 1050. CrossRef - A Rare Case of Recurrent Parathyroid Adenomas After Initial Parathyroidectomy
Grant N Schalet, Luke Vincent, Carl Eguez, Gerardo Diaz, Mark S Shachner
Cureus.2023;[Epub] CrossRef - Surgical treatment of tertiary hyperparathyroidism: does one fit for all?
Claudio Casella, Claudio Guarneri, Manuela Campanile, Xavier Adhoute, Pier Paolo Gelera, Riccardo Morandi
Frontiers in Endocrinology.2023;[Epub] CrossRef - A >50% Intraoperative Parathyroid Hormone Decrease Into Normal Reference Range Predicts Complete Excision of Malignancy in Patients With Parathyroid Carcinoma
Valerie L. Armstrong, Tanaz M. Vaghaiwalla, Cima Saghira, Cheng-Bang Chen, Yujie Wang, Johan Anantharaj, Mehmet Ackin, John I. Lew
Journal of Surgical Research.2023;[Epub] CrossRef - Variation in parathyroid adenoma size in patients with sporadic, primary hyperparathyroidism: small gland size does not preclude single gland disease
Sophie Dream, Tina W. F. Yen, Kara Doffek, Douglas B. Evans, Tracy S. Wang
Langenbeck's Archives of Surgery.2022; 407(5): 2067. CrossRef - Role and Recent Trend of Intraoperative Parathyroid Hormone Monitoring During Parathyroidectomy in Patients With Primary Hyperparathyroidism
Dongbin Ahn, Ji Hye Kwak
Korean Journal of Otorhinolaryngology-Head and Neck Surgery.2022; 65(5): 253. CrossRef - Parathyroid Adenoma: Rare Cause of Acute Recurrent Pancreatitis
Shikha Mahajan, Alka Kumar, Vivek Aggarwal, Vikas Jain, Vipul Baweja, Ajay Ajmani, Diplomate CBNC, Fellow EBNM LNU
Annals of Pediatric Gastroenterology and Hepatology.2022; 2(3-4): 9. CrossRef - Long-term outcome of surgical techniques for sporadic primary hyperparathyroidism in a tertiary referral center in Belgium
Klaas Van Den Heede, Amélie Bonheure, Nele Brusselaers, Sam Van Slycke
Langenbeck's Archives of Surgery.2022; 407(7): 3045. CrossRef - Contribution of intraoperative parathyroid hormone monitoring to the surgical success in minimal invasive parathyroidectomy
Ismail Ethem Akgün, Mehmet Taner Ünlü, Nurcihan Aygun, Mehmet Kostek, Mehmet Uludag
Frontiers in Surgery.2022;[Epub] CrossRef - Surgery for primary hyperparathyroidism
Murilo Catafesta das Neves, Rodrigo Oliveira Santos, Monique Nakayama Ohe
Archives of Endocrinology and Metabolism.2022; 66(5): 678. CrossRef - Використання інтраопераційного моніторингу рівня паратиреоїдного гормону в мінімально інвазивній хірургії щитоподібної та паращитоподібних залоз
S.V. Chernyshov, A.V. Tymkiv, A.V. Vovkanych, I.I. Komisarenko
Endokrynologia.2022; 27(4): 311. CrossRef - Diagnostic Values of Intraoperative (1-84) Parathyroid Hormone Levels are Superior to Intact Parathyroid Hormone for Successful Parathyroidectomy in Patients With Chronic Kidney Disease
Fangyan Xu, Yaoyu Huang, Ming Zeng, Lina Zhang, Wenkai Ren, Hanyang Qian, Ying Cui, Guang Yang, Wenbin Zhou, Shui Wang, Hui Huang, Huimin Chen, Yujie Xiao, Xueyan Gao, Zhanhui Gao, Jing Wang, Cuiping Liu, Jing Zhang, Baiqiao Zhao, Anning Bian, Fan Li, Hui
Endocrine Practice.2021; 27(11): 1065. CrossRef - Delayed Calcium Normalization after Successful Parathyroidectomy in Primary Hyperparathyroidism
Iván Emilio de la Cruz Rodríguez, Elsy Sarahí García Montesinos, María Fernanda Rodríguez-Delgado, Guadalupe Vargas Ortega, Lourdes Balcázar Hernández, Victoria Mendoza Zubieta, Victor Hernández Avendaño, Baldomero González Virla, Micha�l R. Laurent
Case Reports in Endocrinology.2021; 2021: 1. CrossRef - Parathyroid Surgery
Aditya S. Shirali, Uriel Clemente-Gutierrez, Nancy D. Perrier
Neuroimaging Clinics of North America.2021; 31(3): 397. CrossRef - Focused parathyroidectomy without intraoperative parathyroid hormone measurement in primary hyperparathyroidism: Still a valid approach?
Shelby Holt
Surgery.2021; 170(6): 1860. CrossRef - Response to the Comment on “Risk Factors of Redo Surgery After Unilateral Focused Parathyroidectomy – Conclusions From a Comprehensive Nationwide Database of 13,247 Interventions Over 6 Years”
Robert Caiazzo, Camille Marciniak, Francois Pattou
Annals of Surgery.2021; 274(6): e861. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite