
Articles
- Page Path
- HOME > Endocrinol Metab > Volume 28(2); 2013 > Article
-
Case ReportTransformation of Nonfunctioning Pancreatic Neuroendocrine Carcinoma Cells into Insulin Producing Cells after Treatment with Sunitinib
- Jung Hun Ohn1, Yeong Gi Kim1, Se-Hoon Lee2, Hye Seung Jung1
-
Endocrinology and Metabolism 2013;28(2):149-152.
DOI: https://doi.org/10.3803/EnM.2013.28.2.149
Published online: June 18, 2013
1Division of Endocrinology and Metabolism, Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea.
2Division of Hematology and Medical Oncology, Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea.
- Corresponding author: Hye Seung Jung. Division of Endocrinology and Metabolism, Department of Internal Medicine, Seoul National University College of Medicine, 101 Daehak-ro, Jongno-gu, Seoul 110-744, Korea. Tel: +82-2-2072-0240, Fax: +82-2-762-9662, junghs@snu.ac.kr
• Received: February 28, 2013 • Accepted: April 17, 2013
Copyright © 2013 Korean Endocrine Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,129 Views
- 35 Download
- 13 Crossref
ABSTRACT
- We report a rare case of severe hypoglycemia after sunitinib treatment for pancreatic neuroendocrine carcinoma. We describe the initial clinical presentation, laboratory results, pathologic findings, and managment in a patient with a nonfunctioning pancreatic neuroendocrine carcinoma with liver metastases who developed life threatening hypoglycemia after 2 months of sunitinib therapy. A 46-year-old woman presented to the emergency department with loss of consciousness from hypoglycemia. Serum C-peptide and insulin levels at fasting state revealed that the hypoglycemia resulted from endogenous hyperinsulinemia. She had been diagnosed with nonfunctioning pancreatic neuroendocrine carcinoma based on a biopsy of metastatic cervical lymph node and was being treated with sunitinib, a small molecule tyrosine kinase inhibitor. Immunohistochemical stain of the metastatic liver mass demonstrated that the initially nonfunctioning neuroendocrine carcinoma cells had changed into insulin-producing cells after sunitinib therapy. Transarterial chemoembolization of the liver masses and systemic chemotherapy with streptozotocin/adriamycin relieved the hypoglycemia. A nonfunctioning pancreatic neuroendocrine carcinoma was transformed into an insulin-producing tumor after treatment with sunitinib, causing endogenous hyperinsulinemia and severe hypoglycemia.
- Sunitinib is a small molecule multitargeted tyrosine kinase inhibitor currently used for the treatment of cancer. This class of drugs has also been reported to have antidiabetic effects [1-3], but the mechanism has not been elucidated. Here we describe a patient with a nonfunctioning pancreatic neuroendocrine carcinoma with liver metastasis, who developed life-threatening hypoglycemia after treatment with sunitinib. Histological examination of the metastatic mass in the liver suggested that the nonfunctioning neuroendocrine cells were converted into insulin-producing cells, causing hyperinsulinemia and severe hypoglycemia.
INTRODUCTION
- A 46-year-old woman was carried to the emergency room with sudden loss of consciousness before breakfast. During transfer in the ambulance, her blood glucose level was measured as 20 mg/dL. After intravenous infusion of dextrose solution, she regained consciousness.
- Her medical history included a 7-mm size neuroendocrine carcinoma in the pancreas (Fig. 1A), with metastases to retroperitoneal lymph nodes, left supraclavicular lymph nodes and liver (Fig. 1B). The patient had received this diagnosis 4 months prior, after presenting with right flank pain. Needle biopsy and immunohistochemical (IHC) staining of the supraclavicular lymph node had been positive for CD56, chromogranin, and synaptophysin, and negative for glucagon and insulin. One month later, she started taking sunitinib 37.5 mg per day because the disease progressed and the right flank pain increased. After 2 months of sunitinib treatment she felt severe fatigue from which she was diagnosed with hypothyroidism, a common adverse event of sunitinib. She began levothyroxine, but even after normalization of thyroid hormone levels, she experienced intermittent weakness, dizziness, and hunger. To relieve fatigue and hunger, she increased oral intake and experienced weight gain of 10 kg over a month. Her medications included oxycodone to relieve flank pain and famotidine for epigastric soreness. She reported having no personal or family history of thyroid disease or diabetes mellitus.
- On physical examination, she appeared well. Her vital signs were within the normal range, height 156.5 cm and body weight 53 kg. There were two palpable, hard, and nontender lymph nodes of less than 1 cm each in the left supraclavicular area. Goiter was not found. She had tenderness in the right flank on percussion, but hepatosplenomegaly was not noted. Grade 1 hand-foot syndrome (mild erythema), a skin-related side effect of sunitinib was observed. The blood cell count, urinalysis, and serum chemistry and electrolytes were within normal range. A1c at admission was 5.6%. An electrocardiogram revealed a normal sinus rhythm and chest X-ray showed no abnormality. Computed tomography of the abdomen demonstrated an increase in the size of the liver mass from 1.8 to 2.8 cm.
- Overnight fasting plasma glucose was 16 mg/dL with C-peptide and insulin levels of 6.1 ng/mL and 27.2 µIU/mL, respectively. These inappropriately elevated fasting insulin and C-peptide levels compared to the glucose level confirmed that the patient's hypoglycemia resulted from endogenous hyperinsulinemia. Differential diagnosis of endogenous hyperinsulinemia was based on negative titers for insulin antibody and insulin receptor antibody. We performed a liver biopsy to obtain metastatic tissue, and the histologic examination revealed diffuse infiltration of the cancer cells in the liver. IHC staining positive for CD56, chromogranin, and synaptophysin confirmed metastatic neuroendocrine carcinoma. In addition, the metastatic lesion in the liver which had been negative at the initial diagnosis (Fig. 2A) was strongly positive for insulin (Fig. 2B). We concluded that the nonfunctional neuroendocrine carcinoma that metastasized to the liver changed into an insulin-producing tumor after 2 months of administration of sunitinib.
- Since sunitinib may have played a role in the transformation, it was discontinued. However, even with frequent dietary intake, the patient required more than 500 g of glucose per day via the central vein to prevent hypoglycemia. High-dose glucocorticoid and glucagon administration were not effective in relieving the severe hypoglycemia. Eighteen days after discontinuation of sunitinib, severe hypoglycemia persisted and she underwent transarterial chemoembolization (TACE) for the metastatic lesions in the left lobe of her liver. TACE showed extensive and multiple staining of liver nodules, which suggested successful embolization. Intravenous glucose infusion was slowly tapered to 200 g per day during the 2 weeks after TACE. Then a β-cell toxin, streptozotocin (500 mg/m2), and adriamycin (50 mg/m2) were administrated intravenously. Intravenous glucose infusion was stopped 1 week after this infusion. The patient underwent another round of TACE for the right lobe of the liver and intravenous streptozotocin/adriamycin, and she was successfully discharged. One month after the final treatment, her fasting blood glucose was 101 mg/dL. Local control of metastatic carcinoma and systemic administration of β-cell toxin had reversed her severe hypoglycemia.
CASE REPORT
- Generally, tumorous conditions that induce endogenous hyperinsulinism such as insulinoma and nesidioblastosis cause clinical hypoglycemia even for small tumors. Therefore, it is unlikely that the slight increase in tumor burden in the liver in the current case had caused conversion of "preclinical" insulinoma into clinical insulinoma. The patient's liver metastases did not impair liver function, so liver function did not contribute to the hypoglycemia. She developed severe hypoglycemia from endogenous hyperinsulinemia after treatment with sunitinib without initial evidence of insulinoma or impaired liver function.
- IHC staining for insulin in tumor specimens before and after sunitinib treatment suggests that neuroendocrine carcinoma cells were transformed from nonfunctioning to insulin-producing cells after treatment with sunitinib. This hypothesis is further supported by the fact that she recovered from severe hypoglycemia after controlling metastatic tumors with TACE and streptozotocin. However, we should note that her supraclavicular lymph node was biopsied at initial diagnosis of pancreatic neuroendocrine carcinoma because it was easily accessible. In contrast, liver tissue was obtained after use of sunitinib due to significant progression of liver metastases. Our findings suggested that the metastatic liver mass turned to producing insulin upon sunitinib treatment, but we could not rule out production of insulin by the same liver metastatic tissue before sunitinib treatment because pretreatment liver metastatic tissue was not available.
- We previously published a case of sunitinib-induced hypoglycemia occurring in nonfunctioning pancreatic neuroendocrine carcinoma with liver metastasis [4]. In that case, we identified endogenous hyperinsulinism but did not attempt to examine insulin production by tumor cells because the hypoglycemia resolved after treatment with a small dose of prednisolone. Vashi et al. [5] recently reported a similar rare case of transformation from nonfunctioning neuroendocrine tumor into insulin-producing tumor, where the patient had liver metastases. However, hypoglycemia was not ascribed to sunitinib treatment as various chemotherapeutic regimens had been used. In our case, the patient developed severe hypoglycemia after treatment with only sunitinib, with the exception of thyroid hormone which has no previous report of causing hypoglycemia. The similar characteristics of nonfunctioning pancreatic neuroendocrine carcinoma with liver metastases in all these cases suggest that a common mechanism might exist, such as the milieu of liver tissue in which the neuroendocrine carcinoma is embedded.
- The molecular mechanism of the glucose-lowering effect of sunitinib has not been elucidated. Several in vitro and in vivo experiments have suggested that imatinib, another kind of small molecule tyrosine kinase inhibitor, is involved in the autoimmune process, β-cell protection, and insulin sensitivity [6-10]. The platelet-derived growth factor signaling pathway, through which sunitinib works, was recently shown to control age-dependent β-cell proliferation in mouse and human pancreatic islets [11]. Further studies are warranted to understand the molecular mechanism of neuroendocrine cell fate to produce insulin by sunitinib.
- In conclusion, this case and a review of the literature suggest that the use of sunitinib in a patient with pancreatic neuroendocrine carcinoma with liver metastases can bring about hypoglycemia, which could be lethal. Considering the possibility of such a serious adverse effect, we recommend that oncologists carefully monitor hypoglycemic symptoms and blood glucose levels of patients treated with sunitinib. The possibility of transformation of neuroendocrine cells into insulin-producing cells by sunitinib would provide a novel way of manipulating β-cell fate.
DISCUSSION
-
Acknowledgements
- This study was supported by a grant from the Innovative Research Institute for Cell Therapy (A062260) by the Ministry of Health and Welfare, Republic of Korea.
ACKNOWLEDGMENTS
- 1. Billemont B, Medioni J, Taillade L, Helley D, Meric JB, Rixe O, Oudard S. Blood glucose levels in patients with metastatic renal cell carcinoma treated with sunitinib. Br J Cancer 2008;99:1380–1382. ArticlePubMedPMCPDF
- 2. Mokhtari D, Welsh N. Potential utility of small tyrosine kinase inhibitors in the treatment of diabetes. Clin Sci (Lond) 2009;118:241–247. ArticlePubMedPDF
- 3. Templeton A, Brandle M, Cerny T, Gillessen S. Remission of diabetes while on sunitinib treatment for renal cell carcinoma. Ann Oncol 2008;19:824–825. ArticlePubMedPDF
- 4. Lee Y, Jung HS, Choi HJ, Kim MJ, Kim TM, Park KS, Kim SY. Life-threatening hypoglycemia induced by a tyrosine kinase inhibitor in a patient with neuroendocrine tumor: a case report. Diabetes Res Clin Pract 2011;93:e68–e70. ArticlePubMed
- 5. Vashi PG, Gupta D, Dahlk S. A unique case of a nonfunctional metastatic pancreatic neuroendocrine tumor transforming into an insulin-secreting tumor with an unusual clinical course. Pancreas 2011;40:781–784. ArticlePubMed
- 6. Hagerkvist R, Jansson L, Welsh N. Imatinib mesylate improves insulin sensitivity and glucose disposal rates in rats fed a high-fat diet. Clin Sci (Lond) 2008;114:65–71. ArticlePubMedPDF
- 7. Hagerkvist R, Makeeva N, Elliman S, Welsh N. Imatinib mesylate (Gleevec) protects against streptozotocin-induced diabetes and islet cell death in vitro. Cell Biol Int 2006;30:1013–1017. ArticlePubMed
- 8. Hagerkvist R, Sandler S, Mokhtari D, Welsh N. Amelioration of diabetes by imatinib mesylate (Gleevec): role of beta-cell NF-kappaB activation and anti-apoptotic preconditioning. FASEB J 2007;21:618–628. ArticlePubMed
- 9. Han MS, Chung KW, Cheon HG, Rhee SD, Yoon CH, Lee MK, Kim KW, Lee MS. Imatinib mesylate reduces endoplasmic reticulum stress and induces remission of diabetes in db/db mice. Diabetes 2009;58:329–336. ArticlePubMedPMC
- 10. Louvet C, Szot GL, Lang J, Lee MR, Martinier N, Bollag G, Zhu S, Weiss A, Bluestone JA. Tyrosine kinase inhibitors reverse type 1 diabetes in nonobese diabetic mice. Proc Natl Acad Sci U S A 2008;105:18895–18900. ArticlePubMedPMC
- 11. Chen H, Gu X, Liu Y, Wang J, Wirt SE, Bottino R, Schorle H, Sage J, Kim SK. PDGF signalling controls age-dependent proliferation in pancreatic beta-cells. Nature 2011;478:349–355. ArticlePubMedPMCPDF
References

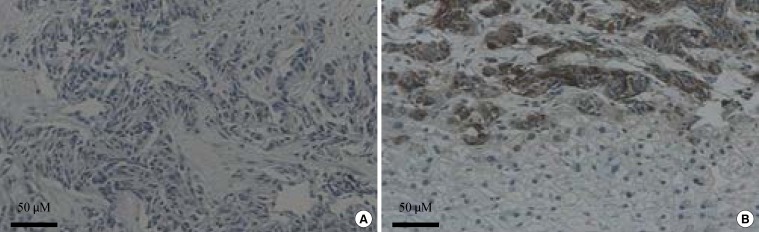
Figure & Data
References
Citations
Citations to this article as recorded by 
- Small Insulinoma Followed-up as an Indolent Pancreatic Tumor: A Case Report
Hiroki Sato, Shozaburo Fujii, Tetsuhiro Okada, Hidemasa Kawabata, Yuki Kamikokura, Mikihiro Fujiya
Internal Medicine.2024;[Epub] CrossRef - A Case of a Metastatic Pancreatic Neuroendocrine Tumor: A Surgical Conundrum Wrapped in Functionality's Embrace
Adam Mylonakis, Michail Vailas, Panagiotis Sakarellos, Lysandros Karydakis, Eleandros Kyros, Spyridon Davakis, Alexandros Papalampros, Evaggelos Felekouras
Cureus.2024;[Epub] CrossRef - Malignant Insulinoma Arising From Nonfunctioning Pancreatic Neuroendocrine Tumor
Ritodhi Chatterjee, Basim Ali, Son H. Nguyen, Rui Chen, Yvonne H. Sada
ACG Case Reports Journal.2023; 10(1): e00954. CrossRef - Case Report: Giant insulinoma, a very rare tumor causing hypoglycemia
Georges Tarris, Alexia Rouland, Kévin Guillen, Romaric Loffroy, Anne-Cécile Lariotte, Patrick Rat, Benjamin Bouillet, Haingo Andrianiaina, Jean-Michel Petit, Laurent Martin
Frontiers in Endocrinology.2023;[Epub] CrossRef - Case Reports: Transformation of End-Stage Neuroendocrine Tumors With Uncontrollable Liver Metastasis Into a Novel or Additional Functional Phenotype
Takaomi Kessoku, Noritoshi Kobayashi, Masato Yoneda, Yuki Kasai, Anna Ozaki, Naoki Okubo, Michihiro Iwaki, Takashi Kobayashi, Tsutomu Yoshihara, Yusuke Kurita, Yasushi Honda, Motohiko Tokuhisa, Hiroto Ishiki, Takashi Hibiya, Satoshi Fujii, Atsushi Nakajim
Frontiers in Oncology.2020;[Epub] CrossRef - Transformation of a non-secretory neuroendocrine tumor to insulinoma after treatment with Sunitinib: A case report and review of the literature
Todd Clover, Amrou Abdelkader, Guru Subramanian Guru Murthy
Journal of Oncology Pharmacy Practice.2019; 25(6): 1516. CrossRef - Hyperglycaemia Induced by Novel Anticancer Agents: An Undesirable Complication or a Potential Therapeutic Opportunity?
Rashmi R. Shah
Drug Safety.2017; 40(3): 211. CrossRef - Medical management of secretory syndromes related to gastroenteropancreatic neuroendocrine tumours
Georgios K Dimitriadis, Martin O Weickert, Harpal S Randeva, Gregory Kaltsas, Ashley Grossman
Endocrine-Related Cancer.2016; 23(9): R423. CrossRef - Different Hormonal Expression Patterns Between Primary Pancreatic Neuroendocrine Tumors and Metastatic Sites
Hideyo Kimura, Takao Ohtsuka, Takaaki Fujimoto, Kenjiro Date, Taketo Matsunaga, Ana Ines Cases, Atsushi Abe, Yusuke Mizuuchi, Yoshihiro Miyasaka, Tetsuhide Ito, Yoshinao Oda, Masafumi Nakamura, Masao Tanaka
Pancreas.2016; 45(7): 947. CrossRef - Tyrosine Kinase Inhibitors and Diabetes: A Novel Treatment Paradigm?
Athanasios Fountas, Leonidas-Nikolaos Diamantopoulos, Agathocles Tsatsoulis
Trends in Endocrinology & Metabolism.2015; 26(11): 643. CrossRef - Transformation of nonfunctioning pancreatic tumor into malignant insulinoma after 3 years: an uncommon clinical course of insulinoma
Muyesser Sayki Arslan, Mustafa Ozbek, Melia Karakose, Esra Tutal, Bekir Ucan, Demet Yilmazer, Alper Dilli, Salih Sinan Gultekin, Erman Cakal, Tuncay Delibasi
Archives of Endocrinology and Metabolism.2015; 59(3): 270. CrossRef - Pancreatic neuroendocrine tumors with transformation to insulinoma: an unusual presentation of a rare disease
Avital Nahmias, Simona Grozinsky-Glasberg, Asher Salmon, David J Gross
Endocrinology, Diabetes & Metabolism Case Reports.2015;[Epub] CrossRef - Brief Review of Articles in 'Endocrinology and Metabolism' in 2013
Won-Young Lee
Endocrinology and Metabolism.2014; 29(3): 251. CrossRef
 PubReader
PubReader Cite
Cite


