Effects of Dipeptidyl Peptidase-4 Inhibitors on Hyperglycemia and Blood Cyclosporine Levels in Renal Transplant Patients with Diabetes: A Pilot Study
Article information

Abstract
Background
The use of dipeptidyl peptidase-4 (DPP-4) inhibitors is increasing among renal transplant patients with diabetes. However, the glucose-lowering efficacies of various DPP-4 inhibitors and their effects on blood cyclosporine levels have not been fully investigated. We compared the glucose-lowering efficacies of DPP 4 inhibitors and evaluate their effects on the blood levels of cyclosporine in renal transplant recipients with diabetes.
Methods
Sixty-five renal allograft recipients who received treatment with DPP-4 inhibitors (vildagliptin, sitagliptin, or linagliptin) following kidney transplant were enrolled. The glucose-lowering efficacies of the DPP-4 inhibitors were compared according to the changes in the hemoglobin A1c (HbA1c) levels after 3 months of treatment. Changes in the trough levels of the cyclosporine were also assessed 2 months after treatment with each DPP-4 inhibitor.
Results
HbA1c significantly decreased in the linagliptin group in comparison with other DPP-4 inhibitors (vildagliptin –0.38%±1.03%, sitagliptin –0.53%±0.95%, and linagliptin –1.40±1.34; P=0.016). Cyclosporine trough levels were significantly increased in the sitagliptin group compared with vildagliptin group (30.62±81.70 ng/mL vs. –24.22±53.54 ng/mL, P=0.036). Cyclosporine trough levels were minimally changed in patients with linagliptin.
Conclusion
Linagliptin demonstrates superior glucose-lowering efficacy and minimal effect on cyclosporine trough levels in comparison with other DPP-4 inhibitors in kidney transplant patients with diabetes.
INTRODUCTION
Kidney transplantation (KT) has become the treatment of choice for end-stage renal disease [1]. With modern advances in surgical techniques and immunosuppressant medications, life expectancy following KT has increased [1] and controlling chronic metabolic complications such as diabetes mellitus is considered an important medical issue [2].
Dipeptidyl peptidase-4 (DPP-4) inhibitors are new oral glucose-lowering agents that prevent the inactivation of glucagon-like peptide-1 and stimulate insulin secretion in a glucose-dependent manner [3]. Because the efficacies of DPP-4 inhibitors for reducing blood glucose have been demonstrated by multiple clinical trials [34], a rapid increase in their clinical use is anticipated [5]. Although different DPP-4 inhibitors showed similar glucose-lowering efficacies [5], they demonstrated various metabolic and excretory properties. Some are metabolized by the cytochrome P450 3A system [6], and their intestinal absorption and renal excretion might be affected by P-glycoprotein, an efflux transporter involved in the absorption and/or elimination of the drug [7].
Cyclosporine is a calcineurin inhibitor and immunosuppressive agent that is widely used in organ transplants and some autoimmune diseases [89]. However, they have a narrow therapeutic window, and levels below this window are associated with an increased risk for rejection, whereas levels above the window are correlated with side effects such as nephrotoxicity, neurotoxicity, hepatotoxicity, and hypertension [10]. Furthermore, because cyclosporine is mainly metabolized in the liver by the cytochrome P450 3A system, as well as P-glycoprotein substrates [11], various compounds that induce or inhibit the cytochrome P450 3A system or P-glycoprotein may influence the trough concentrations of cyclosporine [1213].
Although the concurrent use of DPP-4 inhibitors and immunosuppressants are expected to increase among organ transplant patients with diabetes mellitus, the glucose-lowering efficacy of various DPP-4 inhibitors and their effects on the concentrations of calcineurin inhibitors have not been fully investigated.
In our current study, we compare the glucose-lowering efficacies of three different DPP-4 inhibitors (vildagliptin, sitagliptin, and linagliptin) and evaluate their effects on the trough levels of cyclosporine in KT recipients with diabetes mellitus.
METHODS
Study subjects
We conducted the retrospective, longitudinal, observational study on patients who underwent KT between 2000 and 2013 at Yonsei University Health System (Seoul, Korea) or Asan Medical Center (Seoul, Korea). Among them, renal allograft recipients with diabetes who initiated treatment with DPP-4 inhibitor (vildagliptin, sitagliptin, and linagliptin) after transplantation were enrolled in this study. All KT recipients in both hospital received triple maintenance therapy which was composed of cyclosporine, mycophenolate mofetil or azathioprine, and corticosteroid. All study patients survived >12 months after transplant.
Lifestyle factors and measurements
Height (m) and weight (kg) were measured while each patient was wearing light clothing without shoes. Body mass index (kg/m2) was calculated as weight in kilograms divided by the square of height in meters. Patients with diabetes were defined as those with a fasting plasma glucose (FPG) ≥7.0 mmol/L, hemoglobin A1c (HbA1c) ≥6.5%, and/or receiving antidiabetic medications at 1 year after transplantation.
After overnight fasting, blood samples were drawn from the antecubital vein in the early morning. Fasting total cholesterol, high density lipoprotein cholesterol, low density lipoprotein cholesterol, and triglyceride levels were measured using the enzymatic colorimetric method (Toshiba Medical System Co., Tokyo, Japan). FPG concentrations were measured using enzymatic colorimetric hexokinase (Toshiba Medical System Co.) methods on the Hitachi 7600 system (Hitachi Co., Tokyo, Japan).
HbA1c was measured using the immunoturbidimetric method on the Cobas Integra 800 System (Roche Diagnostics, Basel, Switzerland). Follow-up HbA1c values were measured after 3 months of treatment with the DPP-4 inhibitors. This system is standardized by the International Federation of Clinical Chemistry and Laboratory Medicine (IFCC); however, National Glycohemoglobin Standardization Program (NGSP) approved this measuring system. This machine automatically converts mmol/mol (IFCC) into % (NGSP).
Cyclosporine trough levels were measured by immunoassay methods using the Dimension EXL 200 Integrated Chemistry System (Asan Medical Center) or the Affinity Column Mediated Immunoassay method using the Dimension RXL Max (Yonsei University Health System). Venous samples were drawn 12 hours after the last dose (i.e., immediately before the next dose) in order to measure the trough levels. Changes in the serum cyclosporine trough levels after 2 months treatment were also assessed. Creatinine was measured using the Jaffe method, and the estimated glomerular filtration rate was calculated using the Modification of Diet in Renal Disease study equation [14].
Statistical analysis
Continuous variables with normal distributions are expressed as the mean±standard deviation. Categorical variables are expressed as percentages (%). The characteristics of the study population (according to the type of DPP-4 inhibitor) were compared using one-way analysis of variance for continuous variables, or the chi-square test for categorical variables. The post hoc analysis was performed using Scheffe's method. Follow up HbA1c values were measured after 3 months of treatment with the DPP-4 inhibitor and compared with the baseline values using paired t tests. All statistical analyses were performed using SPSS version 19.0 (IBM Co., Armonk, NY, USA). P values <0.05 were considered statistically significant.
RESULTS
Sixty-five patients who initiated treatment with DPP-4 inhibitors (vildagliptin, sitagliptin, and linagliptin) after KT were analyzed. Twenty-five of these patients underwent KT at Yonsei University Health System, 40 patients underwent KT at Asan Medical Center. The mean age at the initiation of DPP-4 inhibitor was 52.05±9.76 years, and the mean duration of diabetes was 8.14±7.80 years.
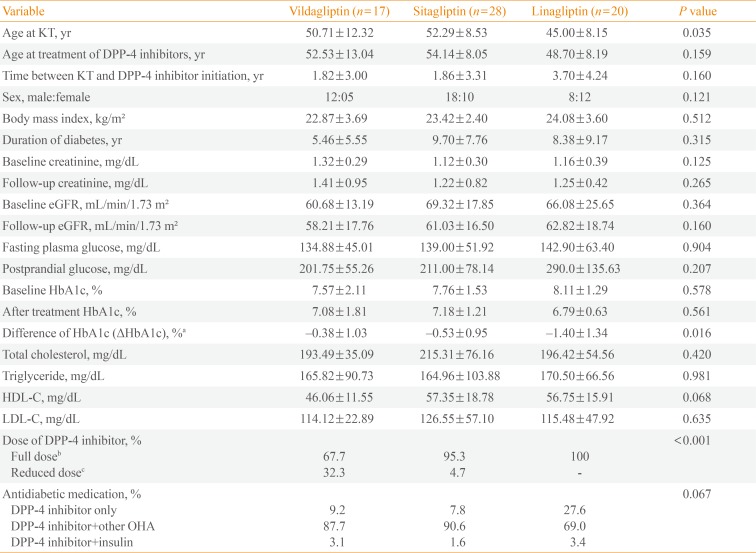
Table 1 shows the clinical and biochemical characteristics of the patients according to the type of DPP-4 inhibitor administered at baseline. Subjects in sitagliptin group were slightly older at the KT than other DPP-4 inhibitor groups (P=0.049). Age at DPP-4 inhibitor initiation was not different among the groups. According to renal function, sitagliptin and vildagliptin doses were adjusted. Both agents were treated with 50 mg once daily in renal insufficient patients. All of the patients in linagliptin group received full dose DPP-4 inhibitor medication. Concurrent anti-diabetic medications were similar among the groups.

Characteristics of Patients and the Effect of DPP-4 Inhibitors on HbA1c
The HbA1c values measured 3 months after treatment with DPP 4 inhibitors were significantly lower in comparison with baseline in all groups (Table 1). When we compared glucose lowering efficacy of DPP-4 inhibitors through the changes in HbA1c from baseline to 3 months of treatment, the levels of HbA1c decreased significantly in the linagliptin group compared with other DPP-4 inhibitor groups (vildagliptin –0.38%±1.03%, sitagliptin –0.53%±0.95%, and linagliptin –1.40±1.34; P=0.016). Even after excluding the patients receiving insulin therapy, the level of HbA1c significantly decreased in the linagliptin group (data not shown).
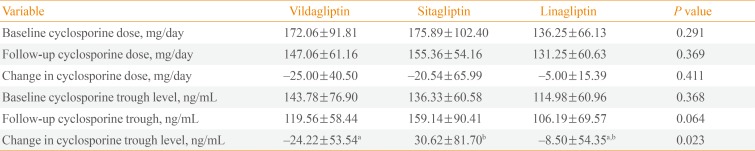
Although there were no differences in baseline cyclosporine doses and blood levels, cyclosporine trough levels were significantly increased in the sitagliptin group (30.62±81.70 ng/mL) in comparison with the vildagliptin group (–24.22±53.54 ng/mL, P=0.031) (Table 2, Fig. 1). Cyclosporine trough levels were minimally changed in patients with linagliptin (–8.50±54.35 ng/mL). There was no difference of change in cyclosporine dose among the three groups (P=0.411) (Table 2, Fig. 1).

Changes in Administered Doses and Trough Levels of Cyclosporine after 2 Months' Treatment of Dipeptidyl Peptidase-4 Inhibitors

Change in cyclosporine trough level. aVildagliptin vs. sitagliptin, P=0.036; vildagliptin vs. linagliptin, P=0.780; sitagliptin vs. linagliptin, P=0.149.
DISCUSSION
In this observational longitudinal study, we found that linagliptin showed a better glucose-lowering efficacy in comparison with other DPP-4 inhibitors in renal allograft recipients with type 2 diabetes. Furthermore, after 2 months of treatment with DPP-4 inhibitors, patients in the sitagliptin group demonstrated increased serum cyclosporine trough levels in comparison with the vildagliptin group.
Hyperglycemia is associated with adverse long-term outcomes in renal allograft recipients with diabetes [151617], and glycemic control is an important factor for preventing allograft loss [16] and reducing patient mortality [17]. Recent data demonstrated that impaired insulin secretion, rather than increased insulin resistance, played an important role in the development of diabetes in KT recipients [18], which indicated that the anti-diabetic agents that preserve or even improve pancreatic β-cell function may be beneficial for glycemic control in organ transplant patients [18]. In previous studies, DPP-4 inhibitors demonstrated protective effects toward pancreatic β-cell survival [1920]. Furthermore, because several studies showed that DPP-4 inhibitors can be safely administered to patients with renal insufficiency at low risk for hypoglycemia [321], increasing use of these medications in KT patients is expected.
Various DPP-4 inhibitors showed similar efficacies in terms of lowering HbA1c [5], but their metabolism and excretion demonstrated widely variable properties [6]. Sitagliptin is primarily eliminated in an unchanged form in the urine (79%), and a relatively small portion is metabolized by the hepatic cytochrome P450 3A4 and 2C8 systems [22]. Vildagliptin is extensively metabolized by multiple pathways that are not mediated by cytochrome P450 enzymes [23], and about two-thirds of the drug is excreted as a metabolite through the kidneys [24]. Vildagliptin did not alter the pharmacokinetic of other drugs using P-glycoprotein–mediated transport system [24]. Linagliptin is mainly eliminated in an unchanged form via the feces (84.7%), and renal excretion only accounts for 5.4% of elimination [25].
In our study, linagliptin significantly reduced HbA1c levels in comparison with other DPP-4 inhibitors over the 3-month follow-up period. Furthermore, serum cyclosporine trough levels increased significantly in the sitagliptin group, even though the administered doses of cyclosporine were decreased for 2 months. Cyclosporine is extensively metabolized in the liver by the cytochrome P450 3A system [12], but the DPP-4 inhibitors compared in our present study are not known as inhibitors or inducers of the cytochrome 450 system [6]. Thus, the different effects of the DPP4-inhibitors on blood cyclosporine trough levels might not be explained by the drug interactions that are mediated by the cytochrome P450 system. Recently, clinically significant drug interactions mediated by P-glycoprotein have been described [11]. P-glycoprotein is an efflux transporter found in the enterocytes, hepatocytes, and renal tubular cells [1126]. Regarding the drug interactions between sitagliptin and cyclosporine, Krishna et al. [27] reported that the sitagliptin AUC0-∞ (area under the concentration-time curves from time zero to infinity) increased in healthy male participants due to the inhibitory effects of cyclosporine on intestinal P-glycoprotein. Considering that both sitagliptin and cyclosporine are substrates and inhibitors of P-glycoprotein [62728], sitagliptin might inhibit intestinal P-glycoprotein in a competitive or noncompetitive manner and promote the absorption of cyclosporine, which in turn increases serum cyclosporine trough levels.
Our study had limitations. First, we did not perform a formal pharmacokinetic study, which requires drawing multiple blood samples over the dosing interval. Thus, the trough levels of the calcineurin inhibitors might not have accurately reflected the AUC0-24 values. Second, we only checked the HbA1c and cyclosporine levels at the baseline visit and at the first follow-up visit. Additional measures at multiple time points should make the conclusion more definite. Although dose of cyclosporine had changed with therapeutic dose monitoring within 2 months and dose of cyclosporine was not different among the DPP-4 inhibitor groups, statistically insignificant change in cyclosporine dose could affect the blood cyclosporine levels. However, our study, as a pilot study, has robust feature in that we first compared the glucose-lowering efficacy of DPP-4 inhibitors in renal allograft recipients and evaluated their effects on the blood concentrations of cyclosporine levels.
In conclusion, we found in this pilot study that linagliptin demonstrates superior glucose-lowering efficacy and minimal effect on cyclosporine trough level in comparison with other DPP-4 inhibitors in kidney transplant patients with diabetes. In addition, patients who receive sitagliptin demonstrated significantly increased cyclosporine trough levels through 2 months of treatment. However larger study and follow up study are warranted to get definite conclusion.
ACKNOWLEDGMENTS
This work was financially supported by the "Kiturami" Faculty Research Assistance Program of Yonsei University College of Medicine (no. 6-2012-0148) and the National Research Foundation of Korea, which is funded by the Korean Government (MEST Basic Research Promotion Fund; nos. NRF-2010-013-E0008 and NRF-2012000891).
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.