
Articles
- Page Path
- HOME > Endocrinol Metab > Volume 38(6); 2023 > Article
-
Original ArticleCalcium & bone metabolism Association between Smoking Status and the Risk of Hip Fracture in Patients with Type 2 Diabetes: A Nationwide Population-Based Study
 Keypoint
Keypoint
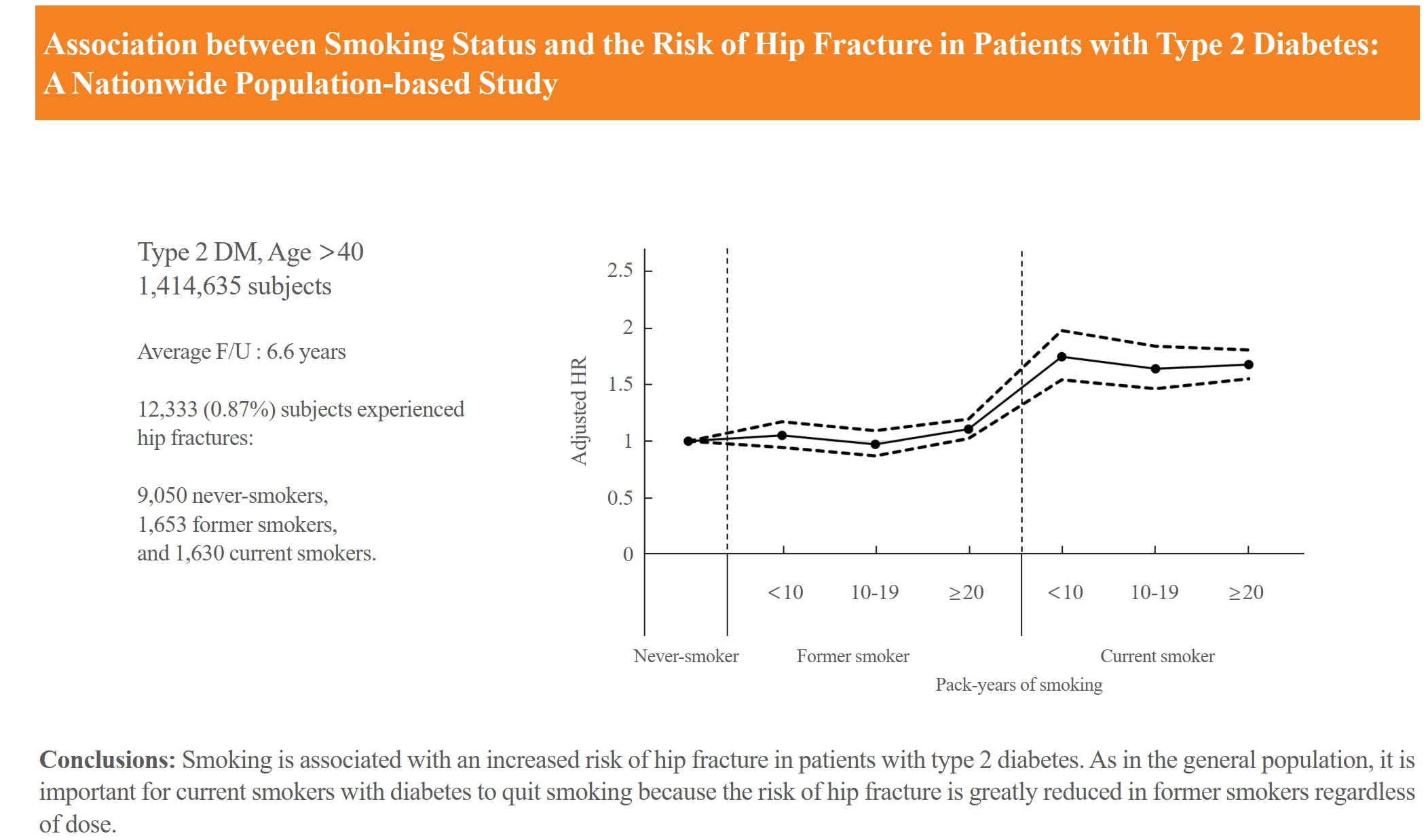
In a Korean study of over 1.4 million adults with type 2 diabetes, current smokers had a significantly higher hip fracture risk (with an adjusted hazard ratio of 1.681) than never-smokers. Former smokers, especially those with a heavy smoking history, also showed increased risk. Notably, female former smokers had risks similar to those of current smokers, while male former smokers resembled never-smokers. Smoking cessation is advised to reduce fracture risk. -
Se-Won Lee1,2
 , Jun-Young Heu3, Ju-Yeong Kim4, Jinyoung Kim5, Kyungdo Han6, Hyuk-Sang Kwon5,7
, Jun-Young Heu3, Ju-Yeong Kim4, Jinyoung Kim5, Kyungdo Han6, Hyuk-Sang Kwon5,7 -
Endocrinology and Metabolism 2023;38(6):679-689.
DOI: https://doi.org/10.3803/EnM.2023.1760
Published online: December 6, 2023
1Department of Orthopedic Surgery, College of Medicine, The Catholic University of Korea, Seoul, Korea
2Department of Orthopedic Surgery, Yeouido St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
3Department of Orthopedic Surgery, Incheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Incheon, Korea
4Department of Orthopedic Surgery, Gyeongsang National University Changwon Hospital, Gyeongsang National University College of Medicine, Changwon, Korea
5Division of Endocrinology and Metabolism, Department of Internal Medicine, Yeouido St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
6Department of Statistics and Actuarial Science, Soongsil University, Seoul, Korea
7Division of Endocrinology and Metabolism, Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea
- Corresponding authors: Kyungdo Han. Department of Statistics and Actuarial Science, Soongsil University, 369 Sangdo-ro, Dongjak-gu, Seoul 06978, Korea Tel: +82-2-820-7025, Fax: +82-2-823-1746, E-mail: hkd917@naver.com
- Hyuk-Sang Kwon. Division of Endocrinology and Metabolism, Department of Internal Medicine, Yeouido St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 10 63-ro, Yeongdeungpo-gu, Seoul 07345, Korea Tel: +82-2-3779-1039, Fax: +82-2-780-3132, E-mail: drkwon@catholic.ac.kr
Copyright © 2023 Korean Endocrine Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,215 Views
- 66 Download
ABSTRACT
-
Background
- Limited longitudinal evidence exists regarding the potential association between smoking status and hip fracture among individuals with type 2 diabetes. We investigated this association using large-scale, nationwide cohort data for the Korean population.
-
Methods
- This nationwide cohort study included 1,414,635 adults aged 40 and older who received Korean National Health Insurance Service health examinations between 2009 and 2012. Subjects with type 2 diabetes were categorized according to their smoking status, amount smoked (pack-years), number of cigarettes smoked per day, and duration of smoking. The results are presented as hazard ratios (HRs) and 95% confidence intervals (CIs) for the associations between smoking status parameters and risk of hip fracture in multivariable Cox proportional hazard regression analysis.
-
Results
- Compared with never-smokers, an increased adjusted HR (aHR) for hip fracture was observed in current smokers (1.681; 95% CI, 1.578 to 1.791), and a comparable aHR for hip fracture was found in former smokers (1.065; 95% CI, 0.999 to 1.136). For former smokers who had smoked 20 pack-years or more, the risk was slightly higher than that for never-smokers (aHR, 1.107; 95% CI, 1.024 to 1.196). The hip fracture risk of female former smokers was similar to that of female current smokers, but the hip fracture risk in male former smokers was similar to that of male never-smokers.
-
Conclusion
- Smoking is associated with an increased risk of hip fracture in patients with type 2 diabetes. Current smokers with diabetes should be encouraged to quit smoking because the risk of hip fracture is greatly reduced in former smokers.
- Smoking increases the risk of fractures at all bone locations according to numerous studies [1,2]. The causal connection between smoking and hip fractures is particularly pronounced in osteoporotic fractures [3-5]. Furthermore, the increasing incidence of hip fractures worldwide is creating medical and financial burdens for society [6-9].
- Smoking is linked to traits that can predict fracture risk without relying on bone mineral density (BMD) measurements at several sites [4,5]. Smoking also increases hip fracture risk by exerting various negative effects on health [7]. According to a study by Ampelas [10], current smokers had a greater risk of hip fracture. Former smokers showed a slightly increased risk of hip fracture compared to never-smokers, and this risk was negatively correlated with the length of time since quitting [10]. Since the harmful effects of smoking are dose-related, cessation may mitigate its toxicity [10-12].
- Diabetes is associated with serious diseases such as heart problems, kidney failure, nerve damage, and eye damage, and some of these complications can lead to amputation of extremities [7]. These complications are more common in people with diabetes who have a history of smoking than in nonsmokers with diabetes [13]. Since that smoking increases the risk of hip fractures in the general population [1], it is plausible to expect that smoking would increase the risk of hip fractures in type 2 diabetes patients [2]. However, although some studies have shown that both type 2 diabetes and smoking are independently related to the risk of hip fracture [13], it is unclear whether smoking is related to hip fracture in patients with type 2 diabetes. Therefore, we investigated the association between smoking and hip fracture risk in this patient population.
INTRODUCTION
- Data source
- We utilized the Korean National Health Insurance System (NHIS) database. It is advised that enrollees receive health exams at least every 2 years. We concentrated on patients with type 2 diabetes among individuals who had health examinations between January 2009 and December 2012 (n=2,746,078). The data for patients with type 2 diabetes were matched with claims data at the time of their health checks and verified by medical information. The operational definitions used in this study are summarized in Supplemental Table S1. The criteria for type 2 diabetes followed those used in the literature [14]: (1) at least one claim per year under International Classification of Diseases, 10th edition (ICD-10) codes E11–14 and at least one claim per year for the prescription of an antidiabetic medication (sulfonylureas, metformin, meglitinides, thiazolidinediones, dipeptidyl peptidase-4 inhibitors, α-glucosidase inhibitors, or insulin) or (2) a fasting glucose level ≥126 mg/dL. Patients who were admitted to the hospital at least once or visited the outpatient clinic at least twice were also included as subjects with type 2 diabetes [14]. Because a definitive hip fracture necessitates hospitalization and surgery, hip fracture was defined as hospitalization with ICD-10 code S72.0 or S72.1. After initial inclusion, we excluded those who did not receive a second health examination within 2 years of their first exam throughout that time period (n=915,219) and those under the age of 40 (n=94,655). Individuals with missing data (n=62,052) were also excluded. Subjects with a history of any fracture from 2002 to the date of their second NHIS medical examination (baseline point) in the period 2009 to 2012 (n=259,517) were excluded since NHIS data were available from 2002. As a result, the total study population included 1,414,635 subjects (Fig. 1). Informed consent was not required because all data submitted by the NHIS are anonymous.
- At the time of the second NHIS medical examination, data on smoking status were collected, and the second NHIS medical examination was used as the baseline point for observation of hip fracture occurrence. The study subjects were followed from the baseline point (the date of their second NHIS medical examination) to the endpoint (hip fracture occurrence) or until December 31, 2018, whichever happened first. The mean length of follow-up was 6.6±1.9 years. This study protocol was reviewed and approved by the Institutional Review Board of Yeouido St. Mary’s Hospital (SC23ZISI0102).
- Smoking status parameters
- The NHIS database provides thorough information about individuals’ demographic traits and lifestyles, which was gathered using standardized self-report questionnaires. The self-report questionnaire data were used to categorize smoking status as follows: those who had smoked more than five packs (100 cigarettes) in their lifetime and continued to smoke were classified as current smokers; those who had smoked more than five packs (100 cigarettes) in their lifetime but stopped smoking were classified as former smokers; and those who had never smoked more than five packs (100 cigarettes) were classified as never-smokers [15-17]. In the self-report questionnaire, former/current smokers recorded their total smoking duration in years and the average daily number of cigarettes smoked. By multiplying the average cigarette consumption per day (packs) by the smoking duration (years), the cumulative lifetime smoking exposure was calculated as pack-years.
- Covariates
- Heavy drinkers were classified as subjects who consumed more than 30 g of alcohol per day on average [18]. Income level was dichotomized into <25% or ≥25%. Regular exercise was defined as intensive physical activity that caused breathing to become faster than usual on at least 3 days a week for at least 20 minutes, or moderate physical activity that caused breathing to become slightly faster than usual on at least 5 days a week for at least 30 minutes [19]. The health checks were performed by trained medical personnel and comprised anthropometric and laboratory measurements. The criteria of comorbidities for hypertension and dyslipidemia followed those previously mentioned in the literature [14].
- Statistical analysis
- All statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA). For continuous variables, baseline parameters regarding smoking status are shown as the means and standard deviations, whereas percentages are used for categorical variables. Analysis of variance was used to compare categorical and continuous data. By dividing the total number of hip fractures by 1,000 person-years, the incidence rate of hip fracture was computed. The results are presented as hazard ratios (HRs) and 95% confidence intervals (CIs) for the associations between smoking status parameters and risk of hip fracture in multivariable Cox proportional hazard regression analysis. For the multivariate analyses, model 1 was not adjusted for any variables; model 2 was adjusted for age, sex, income level, hypertension, dyslipidemia, alcohol consumption status, and exercise level; and model 3 was adjusted for age, sex, income level, hypertension, dyslipidemia, alcohol consumption status, exercise level, fasting glucose level, insulin use, use of ≥3 oral hypoglycemic agents, and duration of diabetes. The tertile categorization of continuous variables was used to visually assess stratified –log(–log) survival curves, and the Harrell and Lee test on Schoenfeld residuals in univariate models was used to verify the proportional hazard assumption [20]. For each category, the HRs and 95% CIs for fractures were estimated using a Cox proportional hazards model. In addition, the subjects were divided into groups based on sex and age, and then subgroup analyses were carried out. There were five age categories: 40–49, 50–59, 60–69, 70–79, and 80 years and over.
METHODS
- Baseline characteristics
- The baseline data of the subjects are shown in Table 1. Current smokers had a higher estimated glomerular filtration rate and serum triglyceride levels (P<0.001). Former smokers had the highest mean waist circumference (P<0.001). Never-smokers showed the highest prevalence of hypertension and dyslipidemia (P<0.001) and lower liver enzyme and serum triglyceride levels (P<0.001). No significant trends were seen in body mass index, height, weight, blood pressure, fasting plasma glucose, total cholesterol, high-density lipoprotein cholesterol, or low-density lipoprotein cholesterol.
- Among the 1,414,635 subjects analyzed, 787,573 (55.7%) were never-smokers, 310,430 (21.9%) were former smokers, and 316,632 (22.4%) were current smokers. More than 90% of the former smokers and current smokers were men. In contrast, the percentage of male never-smokers was approximately 34%. Due to these gender differences between never-smokers, former smokers, and current smokers in baseline characteristics, the baseline characteristics described separately for men and women are shown in Supplemental Table S2.
- Risk of hip fracture according to smoking status, amount smoked (pack-years), number of cigarettes smoked per day, and duration of smoking
- This study examined the risk of hip fracture based on smoking status, pack-years, number of cigarettes smoked per day, and duration of smoking in 1,414,635 participants followed for an average of 6.6 years. During this period, 12,333 (0.87%) subjects experienced hip fractures: 9,050 never-smokers, 1,653 former smokers, and 1,630 current smokers.
- Current smokers had a significantly higher risk of hip fractures than never-smokers, while former smokers did not show a significant difference in risk. The amount smoked, number of cigarettes per day, and duration of smoking did not show a proportional relationship with hip fracture risk for either current or former smokers (Table 2).
- According to smoking status, the adjusted hazard ratio (aHR) for hip fracture was significantly higher in current smokers (aHR, 1.681; 95% CI, 1.578 to 1.791) than in never-smokers. Former smokers did not show a significant difference in hip fracture risk compared to never-smokers (aHR, 1.065; 95% CI, 0.999 to 1.136).
- Regarding the amount smoked, current smokers had an increased hip fracture risk regardless of the number of pack-years: 74.8% for <10 pack-years, 64.2% for 10 to 19 pack-years, and 67.6% for 20 or more pack-years compared to never-smokers. Former smokers also showed a slight increase in risk with 20 or more pack-years (aHR, 1.107; 95% CI, 1.024 to 1.196) (Fig. 2).
- The number of cigarettes smoked per day did not show a proportional increase in hip fracture risk for either current or former smokers. Similarly, the duration of smoking did not have a proportional impact on hip fracture risk for current or former smokers. However, current smokers had a higher risk than neversmokers, especially those who smoked for less than 10 years (aHR, 2.106; 95% CI, 1.677 to 2.644) and those who smoked for 30 or more years (aHR, 1.694; 95% CI, 1.58 to 1.817). Only former smokers who smoked for 30 or more years showed a slightly higher risk (aHR, 1.12; 95% CI, 1.032 to 1.216).
- Subgroup analyses according to age and sex
- Fig. 3 shows subgroup analyses according to age and sex. In the subgroup analysis by sex, the hip fracture risk of female former smokers was similar to that of female current smokers, but the hip fracture risk in male former smokers was similar to that of male never-smokers. In the subgroup analysis by age, the risk of a hip fracture was highest among both current smokers and former smokers in their 40s and showed a tendency to decrease gradually with increasing age. Notably, former smokers aged above 70 years and current smokers aged above 80 years showed hip fracture risks that did not significantly differ from those of individuals who had never smoked.
- The statistical analyses further supported these findings. The P value for interaction by sex was determined to be 0.0012, indicating a significant difference in the effect of smoking on hip fracture risk between males and females. Additionally, the P value for interaction by age group was found to be <0.0001, indicating a highly significant variation in the impact of smoking on hip fracture risk across different age groups.
- Analysis according to smoking maintenance or cessation at the time of the second health exam, based on the current smoker standard in the first health examination
- Table 3 shows the analysis of smoking maintenance or cessation at the time of the second health examination based on the current smoker standard in the first health examination. Contrary to our expectations, among the smokers at the first health examination, there was no significant difference in the values of adjusted model 3 between those who quit smoking and those who continued smoking.
RESULTS
- In this large population-based cohort study involving adults aged 40 and above with type 2 diabetes, we examined the link between smoking and an increased risk of hip fractures. Our results revealed a clear connection between current smoking and an increased risk of hip fractures, highlighting the need for interventions to help individuals with diabetes quit smoking. For former smokers with a smoking history exceeding 20 pack-years, the risk of hip fracture was slightly higher than that for never-smokers (aHR, 1.107; 95% CI, 1.024 to 1.196), indicating a persistent impact of smoking on bone health.
- Diabetes is an endocrine disorder that affects all body systems and produces various complications [21]. The fact that type 1 diabetes patients have lower BMD and an increased risk of hip fracture is well known [22,23]. A few studies have also reported that type 2 diabetes increases the risk of hip fracture, but its association seems weaker than that of type 1 diabetes [24]. Several [25-28], but not all [29,30], previous studies have found that patients with type 2 diabetes are at a higher risk of hip fractures than individuals without diabetes, despite having higher BMD. Even prediabetes may be associated with an increased risk of hip fracture [8].
- Smoking increases the incidence of bone fracture at all skeletal locations, according to earlier studies [1,3,4,7,12,15,17,18,31-34]. Inter alia, cigarette smoking is particularly associated with osteoporotic hip fracture [35]. A significant cohort study that tracked 116,229 female nurses for 12 years found that the relative risk of hip fracture was 1.6 times higher in women who smoked 25 or more cigarettes per day than in never-smokers [36]. After adjusting for age, BMD, and BMI, a meta-analysis of 10 large cohort studies also showed that smoking was the only factor that affected fracture risk [1,37].
- In this study, current smoking was associated with an increased incidence of hip fractures in a population of type 2 diabetes patients. We found no dose-response relationship between the risk of hip fracture and the duration or amount of smoking in either former or current smokers, which was contrary to both expectations and a previous population study of women with diabetes, which reported a very high risk of fractures in heavy smokers [38]. One possibility is that the survey used to record smoking amounts and duration might not have perfectly reflected the actual time someone smoked. People might not remember accurately or might change their smoking habits over time. Additionally, smoking’s effects on bones could be influenced by various factors beyond just how much or how long someone smokes. Genetics, lifestyle, and other health factors might all come into play [37]. In addition, because smoking is generally a socially and medically stigmatized behavior, smokers tend to underreport their smoking status [39]. Therefore, self-report questionnaires may have limitations in determining smoking status. Additionally, since the follow-up period was relatively short, at 6.6 years, smoking cessation may be too short to affect the outcomes for former smokers.
- In the subgroup analysis, we found a significant association with age and sex in the relationship between smoking status and hip fracture risk. The trends in age and sex suggest that in women, a younger age was associated with a greater impact of smoking on hip fracture risk. The subgroup analysis by sex showed that the effect of smoking status on hip fracture risk was significantly stronger in women than in men (Fig. 3). The hip fracture risk of female former smokers was similar to that of female current smokers, whereas the hip fracture risk of male former smokers was similar to that of male never-smokers. This result is consistent with previous studies finding that women were more sensitive than men to the increased fracture risk caused by smoking [5,31]. According to previous studies, 19% to 37% of hip fractures in women are estimated to be caused by tobacco smoking [5,31]. In the present subgroup analysis by age, the risk of hip fracture was highest in current and former smokers in their 40s, and the risk showed a tendency to decrease gradually with increasing age. Former smokers older than 70 years and current smokers older than 80 years showed a risk of hip fracture that did not show a statistically significant difference from that of never-smokers (Fig. 3). One possible explanation for why the hip fracture risk was not significantly higher in older current smokers compared to never-smokers is that the effect of smoking on bone density may be attenuated by other factors that are more prevalent or influential in old age, such as osteoporosis, frailty, comorbidity, medication use, or nutritional status [37]. Another possible explanation is that the survey used to record smoking amounts and duration might not perfectly reflect the actual time someone has smoked [39]. People might not remember accurately or might change their smoking habits over time. This underreporting may vary by age. One study compared self-reported smoking status with cotinine testing in firefighters and reported that self-reported accuracy decreased with advancing age [39]. This may be due to older smokers’ negative attitudes toward smoking or because of health problems that have led them to try to hide their smoking status.
- Table 3 shows the unexpected finding that quitting smoking within 2 years of the first health examination did not significantly reduce hip fracture risk. Among first-time smokers, the difference in hip fracture risk between those who quit later and those who continued smoking was minimal. Long-term abstinence from smoking generally lowers the risk of hip fracture, but our study suggests that short-term abstinence from smoking may not bring the same benefits. In one previous study, short-term abstinence (less than 4 years) did not show a statistically significant reduction in the risk of fracture requiring hospitalization, unlike long-term abstinence (>4 years) [40]. This is a similar conclusion to that of our study (Table 3), in which the risk of hip fracture did not significantly decrease even among smokers within 2 years. Another study found that approximately 60% of quitters resumed smoking within 6 to 12 months [41]. It is possible that some of the short-term quitters in our study resumed smoking during the follow-up period, diluting the positive effects of 2 years of abstinence on hip fracture risk.
- The lower risk of hip fracture found in former smokers implies that quitting smoking can reduce the risk of hip fracture [5,7,34]. Current education for patients with type 2 diabetes who already have or may develop diabetic complications mainly focuses on lifestyle modifications, including weight reduction and exercise. When providing type 2 diabetes patients with advice on preventing diabetic complications, smoking cessation should also be addressed. The Task Force on Community Preventive Services recommends several evidence-based tobacco therapies, one of which is consistent quitting messages from healthcare professionals to people who use tobacco [35,42]. Our findings highlight the significance of physician education for patients with type 2 diabetes who smoke, in addition to osteoporosis screening and osteoporotic hip fracture prevention. Especially for smokers with type 2 diabetes who are female or young, the risk of hip fracture from smoking persists even after they quit smoking. Thus, particular attention should be paid to prevent hip fractures in those patients.
- We believe this is the first study to investigate the association between smoking status and hip fracture risk in subjects with our cohort data. Abundant relevant data allowed us to conduct various subgroup analyses. The analyses were performed after adjusting for a substantial number of confounding variables: age, sex, income level, hypertension, dyslipidemia, alcohol consumption status, exercise level, fasting glucose level, insulin use, use of three or more oral hypoglycemic agents, and duration of diabetes. As Korean society predominantly contains people from a single ethnicity, this nationwide study investigated a homogeneous group.
- Our study has limitations despite those advantages. First, reverse causation, which is an inherent issue in all retrospective cohort designs, may have influenced the findings. To compensate for this possibility, any fracture from 2002 to the date of participants’ second NHIS medical examination (baseline point) in the period from 2009 to 2012 was excluded from the analysis. Second, this study may have been affected by misclassification bias. To exclude individuals with insulin-dependent type 1 diabetes, the ICD-10 code E10, representing type 1 diabetes, was not included in the study. Third, due to the lack of glycated hemoglobin levels in the Korean NHIS database, the exact severity of type 2 diabetes could not be assessed. Fourth, additional research in other ethnic groups is needed to confirm our findings because the subjects we enrolled were solely Korean. Fifth, because we only used the NHIS claims database, not medical or radiologic records, to search for hip fractures, we might have included traumatic hip fractures in our analysis. Sixth, the proportion of male never-smokers (33.99%) was significantly different from that of former smokers (97.84%) and current smokers (95.29%). Due to the impact of the sex ratio, we adjusted the HRs in model 2 and model 3. This is the reason for the large difference between the unadjusted model 1 and the values of models 2 and 3.
- In conclusion, we conclude that smoking is associated with an increased hip fracture risk in patients with type 2 diabetes. As in the general population, it is important for current smokers with diabetes to quit smoking because the risk of hip fracture can be greatly reduced in former smokers regardless of dose. However, the effect of smoking cessation on hip fracture risk was not uniform across different subgroups of patients with diabetes. We found that female and young patients with diabetes had a higher residual risk of hip fracture even after quitting smoking than male and older patients. This suggests that smoking may have a long-lasting impact on bone health in some patients with diabetes and that additional preventive measures may be needed for them. Our findings highlight the importance of individualized smoking cessation counseling and hip fracture prevention strategies for patients with diabetes, especially for those who are female or young.
DISCUSSION
Supplementary Material
Supplemental Table S1.
Supplemental Table S2.
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conception or design: S.W.L., K.H., H.S.K. Acquisition, analysis, or interpretation of data: S.W.L., J.Y.H., J.Y.K., J.K., K.H., H.S.K. Drafting the work or revising: S.W.L. Final approval of the manuscript: S.W.L., J.Y.H., J.Y.K., J.K., K.H., H.S.K.
Article information
-
Acknowledgements
- This work was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. 2021R1A2C2013890).




| Characteristic | Never-smokers (n=787,573) | Former smokers (n=310,430) | Current smokers (n=316,632) | P value | |
|---|---|---|---|---|---|
| Hip fracture | 9,050 (1.15) | 1,653 (0.53) | 1,630 (0.51) | <0.0001 | |
| Age, yr | 61.64±10.17 | 59.47±9.96 | 55.01±9.47 | <0.0001 | |
| Male sex | 267,704 (33.99) | 303,722 (97.84) | 301,716 (95.29) | <0.0001 | |
| BMI, kg/m2 | 24.96±3.34 | 25.01±2.94 | 24.63±3.18 | <0.0001 | |
| Height, cm | 158.52±8.38 | 167.78±6.16 | 168.01±6.61 | <0.0001 | |
| Weight, kg | 63.48±10.64 | 70.92±10.06 | 70.36±11.05 | <0.0001 | |
| Waist circumference, cm | 83.89±8.69 | 87.07±7.67 | 85.96±8.03 | <0.0001 | |
| Income (Q1) | 168,232 (21.36) | 52,102 (16.78) | 63,988 (20.21) | <0.0001 | |
| Hypertension | 485,610 (61.66) | 188,591 (60.75) | 163,159 (51.53) | <0.0001 | |
| Dyslipidemia | 391,767 (49.74) | 136,892 (44.1) | 129,861 (41.01) | <0.0001 | |
| Heavy drinkera | 22,874 (2.9) | 40,228 (12.96) | 56,991 (18) | <0.0001 | |
| Regular exerciseb | 174,356 (22.14) | 96,741 (31.16) | 66,241 (20.92) | <0.0001 | |
| Insulin use | 38,996 (4.95) | 14,113 (4.55) | 11,978 (3.78) | <0.0001 | |
| Duration of diabetes, yr | 4.68±3.96 | 4.25±3.95 | 3.62±3.85 | <0.0001 | |
| Use of three or more oral hypoglycemic agents | 82,489 (10.47) | 30,014 (9.67) | 32,109 (10.14) | <0.0001 | |
| Sulfonylurea | 309,656 (39.32) | 109,119 (35.15) | 105,676 (33.38) | <0.0001 | |
| Metformin | 438,170 (55.64) | 159,534 (51.39) | 149,137 (47.1) | <0.0001 | |
| Meglitinides | 6,216 (0.79) | 2,493 (0.8) | 1,701 (0.54) | <0.0001 | |
| Thiazolidinedione | 31,331 (3.98) | 12,541 (4.04) | 11,527 (3.64) | <0.0001 | |
| Dipeptidyl peptidase-4 inhibitor | 128,815 (16.36) | 50,682 (16.33) | 48,566 (15.34) | <0.0001 | |
| Alpha-glucosidase inhibitor | 57,068 (7.25) | 19,365 (6.24) | 18,087 (5.71) | <0.0001 | |
| SBP, mm Hg | 128.26±15.46 | 128.41±14.52 | 126.71±14.76 | <0.0001 | |
| DBP, mm Hg | 77.62±9.84 | 78.68±9.77 | 78.62±9.97 | <0.0001 | |
| Fasting plasma glucose, mg/dL | 132.1±42.81 | 133.28±41.87 | 138.25±50.2 | <0.0001 | |
| eGFR, mL/min/1.73 m2 | 84.97±35.07 | 85.94±46.46 | 90.66±44.98 | <0.0001 | |
| Total cholesterol, mg/dL | 188.83±40.61 | 184.01±39.5 | 189.94±40.5 | <0.0001 | |
| HDL-C, mg/dL | 51.76±14.93 | 49.79±14.56 | 49.2±15.32 | <0.0001 | |
| LDL-C, mg/dL | 108.1±36.82 | 103.44±35.73 | 105.61±38.16 | <0.0001 | |
| AST | 24.64 (24.62–24.66) | 26.48 (26.44–26.52) | 25.99 (25.95–26.03) | <0.0001 | |
| ALT | 23.3 (23.27–23.33) | 26.67 (26.62–26.72) | 26.4 (26.35–26.46) | <0.0001 | |
| rGTP, mg/dL | 27.12 (27.08–27.16) | 39.26 (39.16–39.36) | 48.18 (48.05–48.32) | <0.0001 | |
| Triglyceride, mg/dL | 127.06 (126.92–127.21) | 134.8 (134.53–135.06) | 155.9 (155.59–156.2) | <0.0001 | |
Values are expressed as number (%), mean±standard deviation, or geometric mean (95% confidence interval).
BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; AST, aspartate transaminase; ALT, alanine transaminase; rGTP, gamma-glutamyltranspeptidase.
a Defined as a person who drinks more than 30 g of alcohol a day on average;
b Defined as high-intensity exercise on more than 3 days a week for at least 20 minutes at a time or moderate-intensity exercise on more than 5 days a week for at least 30 minutes at a time.
Model 1: unadjusted; Model 2: adjusted for age, sex, income level, hypertension, dyslipidemia, alcohol consumption status, and exercise level; Model 3, adjusted for model 2 plus fasting glucose level, insulin use, use of three or more oral hypoglycemic agents, and duration of diabetes.
IR, incidence rate; HR, hazard ratio; CI, confidence interval.
Model 1: unadjusted; Model 2: adjusted for age, sex, income level, hypertension, dyslipidemia, alcohol consumption status, and exercise level; Model 3; adjusted for model 2 plus fasting glucose level, insulin use, use of three or more oral hypoglycemic agents, and duration of diabetes.
IR, incidence rate; HR, hazard ratio; CI, confidence interval.
- 1. Yoon V, Maalouf NM, Sakhaee K. The effects of smoking on bone metabolism. Osteoporos Int 2012;23:2081–92.ArticlePubMedPDF
- 2. Wakasugi M, Kazama JJ, Nitta K, Narita I. Smoking and risk of fractures requiring hospitalization in haemodialysis patients: a nationwide cohort study in Japan. Nephrol Dial Transplant 2022;37:950–9.ArticlePubMedPDF
- 3. Holmberg AH, Johnell O, Nilsson PM, Nilsson JA, Berglund G, Akesson K. Risk factors for hip fractures in a middle-aged population: a study of 33,000 men and women. Osteoporos Int 2005;16:2185–94.ArticlePubMedPDF
- 4. Olofsson H, Byberg L, Mohsen R, Melhus H, Lithell H, Michaelsson K. Smoking and the risk of fracture in older men. J Bone Miner Res 2005;20:1208–15.ArticlePubMed
- 5. Benetos IS, Babis GC, Zoubos AB, Benetou V, Soucacos PN. Factors affecting the risk of hip fractures. Injury 2007;38:735–44.ArticlePubMed
- 6. Rodrigues AM, Caetano-Lopes J, Vale AC, Aleixo I, Pena AS, Faustino A, et al. Smoking is a predictor of worse trabecular mechanical performance in hip fragility fracture patients. J Bone Miner Metab 2012;30:692–9.ArticlePubMedPDF
- 7. Cummings SR, Nevitt MC, Browner WS, Stone K, Fox KM, Ensrud KE, et al. Risk factors for hip fracture in white women. Study of Osteoporotic Fractures Research Group. N Engl J Med 1995;332:767–73.ArticlePubMed
- 8. Park HY, Han K, Kim Y, Kim YH, Sur YJ. The risk of hip fractures in individuals over 50 years old with prediabetes and type 2 diabetes: a longitudinal nationwide populationbased study. Bone 2021;142:115691.ArticlePubMed
- 9. Shao CJ, Hsieh YH, Tsai CH, Lai KA. A nationwide seven-year trend of hip fractures in the elderly population of Taiwan. Bone 2009;44:125–9.ArticlePubMed
- 10. Ampelas DG. Current and former smokers and hip fractures. J Frailty Sarcopenia Falls 2018;3:148–54.ArticlePubMedPMC
- 11. Yang YS, Sohn TS. Smoking as a target for prevention of diabetes. Diabetes Metab J 2020;44:402–4.ArticlePubMedPMCPDF
- 12. Kim JH, Seo DC, Kim BJ, Kang JG, Lee SJ, Lee SH, et al. Association between cigarette smoking and new-onset diabetes mellitus in 78,212 Koreans using self-reported questionnaire and urine cotinine. Diabetes Metab J 2020;44:426–35.PubMed
- 13. Centers for Disease Control and Prevention. Smoking and diabetes [Internet]. Atlanta: CDC; 2022 [cited 2023 Oct 5]. Available from: https://www.cdc.gov/diabetes/library/features/smoking-and-diabetes.html.
- 14. Ko SH, Han K, Lee YH, Noh J, Park CY, Kim DJ, et al. Past and current status of adult type 2 diabetes mellitus management in Korea: a national health insurance service database analysis. Diabetes Metab J 2018;42:93–100.ArticlePubMedPMCPDF
- 15. Yun WJ, Shin MH, Kweon SS, Ryu SY, Rhee JA. Association of smoking status, cumulative smoking, duration of smoking cessation, age of starting smoking, and depression in Korean adults. BMC Public Health 2012;12:724.ArticlePubMedPMCPDF
- 16. Park S, Chun J, Han KD, Soh H, Kang EA, Lee HJ, et al. Dose-response relationship between cigarette smoking and risk of ulcerative colitis: a nationwide population-based study. J Gastroenterol 2019;54:881–90.ArticlePubMedPDF
- 17. Kulak JA, LaValley S. Cigarette use and smoking beliefs among older Americans: findings from a nationally representative survey. J Addict Dis 2018;37:46–54.ArticlePubMed
- 18. Agarwal DP. Cardioprotective effects of light-moderate consumption of alcohol: a review of putative mechanisms. Alcohol Alcohol 2002;37:409–15.ArticlePubMed
- 19. International Physical Activity Questionnaire. Guidelines for data processing and analysis of the International Physical Activity Questionnaire (IPAQ) [Internet]. International Physical Activity Questionnaire Research Committee; 2005 [cited 2023 Oct 5]. Available from: https://www.ipaq.ki.se.
- 20. Kleinbaum DG, Klein M. Survival analysis; 2nd ed. New York: Springer; 2005.
- 21. Botella Martinez S, Varo Cenarruzabeitia N, Escalada San Martin J, Calleja Canelas A. The diabetic paradox: bone mineral density and fracture in type 2 diabetes. Endocrinol Nutr 2016;63:495–501.ArticlePubMed
- 22. Chen C, Chen Q, Nie B, Zhang H, Zhai H, Zhao L, et al. Trends in bone mineral density, osteoporosis, and osteopenia among U.S. adults with prediabetes, 2005-2014. Diabetes Care 2020;43:1008–15.ArticlePubMedPDF
- 23. Holmberg AH, Nilsson PM, Nilsson JA, Akesson K. The association between hyperglycemia and fracture risk in middle age: a prospective, population-based study of 22,444 men and 10,902 women. J Clin Endocrinol Metab 2008;93:815–22.ArticlePubMedPDF
- 24. Lee SW, Han K, Kwon HS. Weight change and the risk of hip fractures in patients with type 2 diabetes: a nationwide cohort study. Osteoporos Int 2022;33:1755–67.ArticlePubMedPDF
- 25. Martinez-Laguna D, Tebe C, Javaid MK, Nogues X, Arden NK, Cooper C, et al. Incident type 2 diabetes and hip fracture risk: a population-based matched cohort study. Osteoporos Int 2015;26:827–33.ArticlePubMedPDF
- 26. Hothersall EJ, Livingstone SJ, Looker HC, Ahmed SF, Cleland S, Leese GP, et al. Contemporary risk of hip fracture in type 1 and type 2 diabetes: a national registry study from Scotland. J Bone Miner Res 2014;29:1054–60.ArticlePubMedPMCPDF
- 27. Melton LJ 3rd, Leibson CL, Achenbach SJ, Therneau TM, Khosla S. Fracture risk in type 2 diabetes: update of a population-based study. J Bone Miner Res 2008;23:1334–42.ArticlePubMedPMC
- 28. Lipscombe LL, Jamal SA, Booth GL, Hawker GA. The risk of hip fractures in older individuals with diabetes: a population-based study. Diabetes Care 2007;30:835–41.PubMed
- 29. Ahmed LA, Joakimsen RM, Berntsen GK, Fonnebo V, Schirmer H. Diabetes mellitus and the risk of non-vertebral fractures: the Tromso study. Osteoporos Int 2006;17:495–500.ArticlePubMedPDF
- 30. de Liefde II, van der Klift M, de Laet CE, van Daele PL, Hofman A, Pols HA. Bone mineral density and fracture risk in type-2 diabetes mellitus: the Rotterdam Study. Osteoporos Int 2005;16:1713–20.ArticlePubMedPDF
- 31. Hoidrup S, Prescott E, Sorensen TI, Gottschau A, Lauritzen JB, Schroll M, et al. Tobacco smoking and risk of hip fracture in men and women. Int J Epidemiol 2000;29:253–9.ArticlePubMed
- 32. Hopkins DP, Briss PA, Ricard CJ, Husten CG, Carande-Kulis VG, Fielding JE, et al. Reviews of evidence regarding interventions to reduce tobacco use and exposure to environmental tobacco smoke. Am J Prev Med 2001;20(2 Suppl):16–66.PubMed
- 33. Ward KD, Klesges RC. A meta-analysis of the effects of cigarette smoking on bone mineral density. Calcif Tissue Int 2001;68:259–70.ArticlePubMedPMCPDF
- 34. Hundrup YA, Hoidrup S, Ekholm O, Davidsen M, Obel EB. Risk of low-energy hip, wrist, and upper arm fractures among current and previous users of hormone replacement therapy: the Danish Nurse Cohort Study. Eur J Epidemiol 2004;19:1089–95.ArticlePubMedPDF
- 35. Jenkins MR, Denison AV. Smoking status as a predictor of hip fracture risk in postmenopausal women of northwest Texas. Prev Chronic Dis 2008;5:A09.PubMed
- 36. Cornuz J, Feskanich D, Willett WC, Colditz GA. Smoking, smoking cessation, and risk of hip fracture in women. Am J Med 1999;106:311–4.ArticlePubMed
- 37. Kanis JA, Johnell O, Oden A, Johansson H, De Laet C, Eisman JA, et al. Smoking and fracture risk: a meta-analysis. Osteoporos Int 2005;16:155–62.ArticlePubMedPDF
- 38. Jorgensen L, Joakimsen R, Ahmed L, Stormer J, Jacobsen BK. Smoking is a strong risk factor for non-vertebral fractures in women with diabetes: the Tromso Study. Osteoporos Int 2011;22:1247–53.ArticlePubMedPDF
- 39. Heo HC, Byun YS, Sohn SH, Jo SM, Park SK, Sakong J. Validity assessment of self-reported smoking status in firefighters using the urine cotinine test. Ann Occup Environ Med 2020;32:e2.ArticlePubMedPMCPDF
- 40. Cho IY, Cho MH, Lee K, Park SM, Lee H, Son JS, et al. Effects of smoking habit change on hospitalized fractures: a retrospective cohort study in a male population. Arch Osteoporos 2020;15:29.ArticlePubMedPDF
- 41. Santi SA, Conlon MS, Meigs ML, Davidson SM, Mispel-Beyer K, Saunders DP. Rates of smoking cessation at 6 and 12 months after a clinical tobacco smoking cessation intervention in head and neck cancer patients in Northern Ontario, Canada. Curr Oncol 2022;29:1544–58.ArticlePubMedPMC
- 42. Community Preventive Services Task Force. The community guide [Internet]. Atlanta: CDC; 2023 [cited 2023 Oct 5]. Available from: https://www.thecommunityguide.org/pages/about-community-guide.html.
References
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-



- Related articles
-
- Long-Term Cumulative Exposure to High γ-Glutamyl Transferase Levels and the Risk of Cardiovascular Disease: A Nationwide Population-Based Cohort Study
- Increased Risk of Hip Fracture in Patients with Acromegaly: A Nationwide Cohort Study in Korea
- Coronary Artery Calcium Score as a Sensitive Indicator of Cardiovascular Disease in Patients with Type 2 Diabetes Mellitus: A Long-Term Cohort Study
- Prevalence, Treatment Status, and Comorbidities of Hyperthyroidism in Korea from 2003 to 2018: A Nationwide Population Study
- Predicting the Risk of Insulin-Requiring Gestational Diabetes before Pregnancy: A Model Generated from a Nationwide Population-Based Cohort Study in Korea

