Cardiovascular Impact of Calcium and Vitamin D Supplements: A Narrative Review
Article information

Abstract
Calcium and vitamin D play an important role in mineral homeostasis and the maintenance of skeletal health. Calcium and vitamin D supplements have been widely used for fracture prevention in elderly populations. Many trials have studied the effectiveness and cardiovascular safety of calcium and vitamin D supplementation, with disparate results. In this review, we summarize the most important trials and systematic reviews. There is significant heterogeneity in clinical trial design, differences in the nature of trial outcomes (self-reported vs. verified), prior calcium intake, and trial size. Inconsistent results have been reported concerning the effects of calcium and vitamin D supplementation on cardiovascular outcomes. Most current guidelines recommend calcium intake of up to 1,200 mg daily, preferably from the diet, without concern for cardiovascular risk. Recommendations regarding vitamin D supplementation vary widely. There is compelling evidence from well-conducted randomized trials that modest vitamin D supplementation is safe but does not confer cardiovascular benefit or cardiovascular harm.
INTRODUCTION
Calcium is required for bone mineralization as well as a wide variety of physiologic processes. The skeleton is both essential for muscle attachment, enabling ambulation, and as a source of calcium to maintain homeostasis at times of low enteral calcium availability. The plasma concentration of calcium is maintained by the interplay among intestinal absorption, renal calcium tubular reabsorption, and endocrine factors, primarily parathyroid hormone (PTH) and vitamin D metabolites. Besides its importance for skeletal health, calcium plays roles in cell division, muscle and neurologic function, blood coagulation, exocytosis, and metabolic regulation [1]. Vitamin D metabolites increase the intestinal absorption of calcium, and vitamin D deficiency is associated with decreased calcium absorption with increases in PTH and secondary hyperparathyroidism. Increased PTH increases calcium absorption by stimulating the conversion of 25-hydroxyvitamin D (25-OHD) to 1,25-dihydroxyvitamin D, which in turn acts as a hormone, stimulating intestinal calcium absorption [2]. In addition, increased PTH directly stimulates osteoclastic bone resorption through the receptor activator of NF-κB (RANK) ligand pathway, drawing in calcium from bone and leading to bone loss [2]. Vitamin D is also required for bone mineralization; severe vitamin D deficiency results in osteomalacia, a condition where osteoid remains unmineralized. With age, multiple physiological changes occur and can contribute to calcium and vitamin D insufficiency. Elderly people often consume inadequate calcium, have reduced calcium absorption, and have decreased skin vitamin D production and decreased vitamin D activation in the kidney [3]. Because of these metabolic changes, the elderly may require calcium and/or vitamin D supplementation. However, excessive supplemental calcium and vitamin D intake sometimes occurs in an attempt to maintain skeletal integrity or reverse osteoporosis. Excessive calcium supplementation may lead to bloating, constipation, and an increased risk of nephrolithiasis [4].
There has been controversy in the literature over the past 8 years regarding the cardiovascular safety of calcium supplements, and extensive data have been published in attempts to determine whether this risk exists. This narrative review summarizes the most important randomized controlled trials (RCTs) and systematic reviews that address the cardiovascular safety of calcium and vitamin D supplementation in elderly individuals.
SKELETAL AND EXTRASKELETAL EFFECTS OF CALCIUM AND VITAMIN D
A recent network meta-analysis demonstrated that a combination of calcium and vitamin D was associated with a 19% relative risk (RR) reduction for hip fractures compared to placebo (hazard ratio [HR], 0.81; 95% confidence interval [CI], 0.71 to 0.93); there was no effect on vertebral fractures [5]. Monotherapy with calcium or vitamin D alone was not associated with fracture risk reduction [5]. In one of the earliest controlled trials of calcium and vitamin D, Chapuy et al. [6] in 1992 studied over 3,000 elderly residents in an ambulatory setting in southern France. Participants were randomized to supplementation with 1,200 mg of elemental calcium and 800 IU of vitamin D daily or placebo [6]. The combination of calcium and vitamin D was associated with a 43% reduction in hip fractures compared to placebo. At baseline, the participants were vitamin D-insufficient (serum 25-OHD: 16±11 ng/mL in the intervention group and 13±9 ng/mL in the control) [6]. The Decalyos II study demonstrated the effectiveness of calcium and vitamin D supplementation (1,200 mg of calcium and 800 IU of vitamin D) in vitamin D-deficient subjects in reversing secondary hyperparathyroidism as early as 6 months after initiating supplements [7]. There was no statistically significant difference in the probability of hip and non-vertebral fractures between the placebo arm and the calcium and vitamin D arm [7]. Since calcium and vitamin D are threshold nutrients, calcium supplementation is likely to be most beneficial in individuals with insufficient calcium intake. Individuals with adequate dietary calcium intake are unlikely to benefit from additional supplemental calcium. No additional bone health benefits were observed with vitamin D supplementation in vitamin D-replete community-dwelling individuals. However, it is prudent to recommend vitamin D supplementation in institutionalized and frail older individuals and in patients on osteoporosis treatment, since there is likely a synergy between calcium and vitamin D supplementation and the therapeutic effects of osteoporosis medication. Several randomized trials have shown that vitamin D supplementation leads to a signification reduction in the risk of falls in vitamin D-deficient patients [8-10]. A positive effect of vitamin D supplementation on autoimmune diseases (rheumatoid arthritis [RA], systemic lupus erythematosus [SLE], and multiple sclerosis [MS]) has been observed in animal models [11]. However, in human studies, vitamin D supplementation was associated with a lower risk of developing MS, but not SLE or RA [12]. A RCT by Lappe et al. [13] showed that calcium and vitamin D supplementation did not lead to a decreased risk of cancer in elderly vitamin D-replete women.
On the other hand, excessive calcium supplementation can be associated with a high-risk of nephrolithiasis. The Women’s Health Initiative (WHI) trial showed that a total calcium intake of 2,100 mg per day was associated with a 17% increased risk of kidney stones [14]. Hypercalciuria in this setting depends not only on total calcium intake, but also on the timing of calcium relative to meals, as well as sodium and oxalate intake. It is well established that calcium taken with meals acts as a chelator for oxalate, which interferes with its absorption and urinary excretion [15]. Thus, calcium restriction is not recommended for the prevention of calcium stone formation [15]. The timing of calcium supplementation relative to meals was studied in 32 healthy males. This study showed that calcium carbonate supplementation (either 1 g three times daily with meals or 3 g at bedtime) led to an increase in calciuria compared to baseline, but only calcium taken with meals was associated with a decline of oxalate excretion compared to baseline [16].
EFFECT OF CALCIUM/VITAMIN D SUPPLEMENTATION ON THE CARDIOVASCULAR SYSTEM
Effect of calcium supplementation on the cardiovascular system
Calcium supplementation is usually associated with a small increase in serum calcium and a consequent decrease in serum PTH, with both usually remaining in the normal range. This modest rise in serum calcium is considered unlikely to lead to extraskeletal calcification [17]. Clinical trials of PTH and its analogs in osteoporosis subjects have demonstrated mild transient increases in serum calcium, which do not appear to have detrimental cardiovascular effects [18]. That being said, some observational studies still question the link between transient hypercalcemia, endothelial dysfunction, atherosclerosis, and arterial stiffness [19]. These findings are in line with recent Mendelian randomization studies. These studies take a genetic epidemiological approach to estimate causality and have suggested a positive causal influence of transient increases in serum calcium on increased cardiovascular disease risk, especially for myocardial infarction (MI) [20-23]. However, this increase in cardiovascular disease risk was not observed with higher intake of dietary calcium [24]. Calcium supplementation could have favorable effects on lipids and blood pressure. An RCT examining the effect of calcium supplementation (1 g of calcium citrate) compared to placebo on lipid profiles in 223 postmenopausal females showed that calcium citrate supplementation was associated with a 7% increase in high-density lipoprotein (P=0.01) and a 6% decrease in low-density lipoprotein (P=0.09) at 1 year of follow-up [25]. Other data suggest that transient hypercalcemia and reduction in PTH in subjects taking calcium supplements may be associated with decreased blood pressure [17,26]. A systematic review of 42 trials examining the effect of calcium supplementation on blood pressure showed a reduction in systolic blood pressure by 1.44 mm Hg (95% CI, –2.20 to –0.68; P<0.001) and in diastolic blood pressure of 0.84 mm Hg (95% CI, –1.44 to –0.24; P<0.001) [26]. A study specifically investigating insulin sensitivity and calcium supplementation showed an association of calcium supplementation with increased insulin sensitivity [27]. This was also a finding in the multicenter Insulin Resistance Atherosclerosis Study, which examined the cross-sectional association between calcium intake (mean±standard deviation: 970 mg of elemental calcium±647 mg) and insulin resistance in 1,036 adults without diabetes [27]. Furthermore, plaque rupture in advanced cardiovascular disease is not thought to involve calcium [28]. In a post hoc analysis of nine randomized trials investigating the effect of calcium supplementation on calcium indices (CaI) and atheroma volume (AV), calcium supplementation was associated with an increase in the annualized CaI (odds ratio, 1.15; P=0.004) and no change in AV. Although the authors adjusted for multiple confounders, one of the limitations of this study is that the participants were asked about their “medication use” rather than their “supplement” use [29]. Manson et al. [30] investigated the effect of calcium supplementation (1,000 mg) and vitamin D (400 IU) on the coronary artery calcium (CAC) score in a substudy of the WHI trial. The CAC score was measured at baseline and after 7 years of study in 754 women aged between 50 and 59 years old. There was no significant difference in the CAC score between calcium and vitamin D-supplemented versus non-supplemented patients [30]. The Multi-Ethnic Study of Atherosclerosis was a 10-year observational study of calcium intake in elderly individuals. This study concluded that high total calcium intake was associated with a decreased risk of atherosclerosis, specifically if this was achieved from diet. However, after accounting for total calcium intake, calcium supplements were associated with incident CAC [24]. Interestingly, it has been shown that calcified carotid plaques are less likely to cause symptoms than non-calcified ones, suggesting that calcium can make plaques more stable and less likely to rupture [31]. The potential effects of calcium supplementation on parameters associated with cardiovascular risk are summarized in Fig. 1.
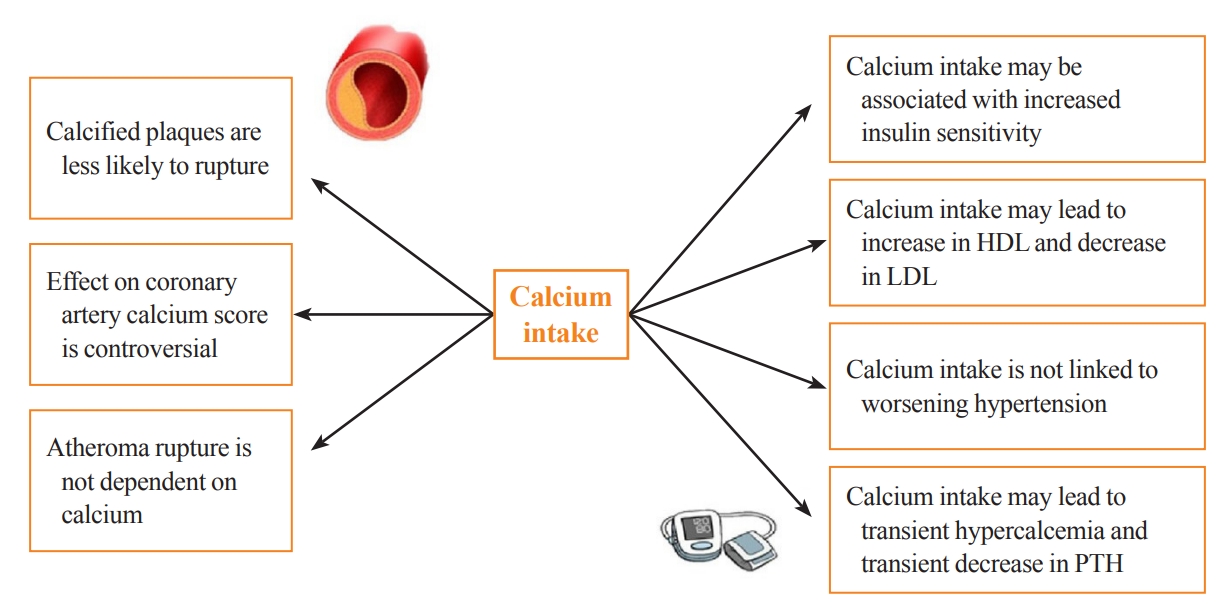
Potential effects of calcium supplementation on parameters associated with cardiovascular risk. HDL, high-density lipoprotein; LDL, low-density lipoprotein; PTH, parathyroid hormone.
Effect of vitamin D supplementation on cardiovascular health
The cutoff to define vitamin D deficiency is controversial, with most guidelines considering a level less than 20 to 30 ng/mL as deficient [32-34]. Around one-third of the global population is affected by vitamin D deficiency when a cutoff of 20 ng/mL is used to define hypovitaminosis D [33]. Multiple conditions can lead to vitamin D deficiency, including low vitamin D intake, inadequate exposure to sun, use of sunscreens, obesity, aging, malabsorption syndromes (such as celiac disease, bariatric surgery, small intestine disorders) liver disease, chronic renal failure, hypoparathyroidism, antiseizure medications, and certain genetic diseases (defective 25-hydroxyvitamin D-1α hydroxylase) [35].
A number of observational studies have reported that subjects with low serum 25-OHD have increased risks of cardiovascular diseases, including MI, congestive heart failure, stroke, peripheral vascular diseases, and mortality [36-41]. A meta-analysis of prospective studies with 6,123 cardiovascular events in 65,994 individuals showed a linear, inverse association between circulating 25-OHD in the range of 8 to 24 ng/mL and the risk of cardiovascular disease with a RR of 1.03 (95% CI, 1.00 to 1.06) per 10 ng/mL decrement in 25-OHD levels [42]. Such observational studies are limited by their inability to prove causality and by the presence of multiple confounding factors [43]. The proposed mechanisms for the cardiovascular effects of low vitamin D are activation of the renin angiotensin aldosterone system, hypercoagulability, increased arterial stiffness, and endothelial dysfunction [43,44].
Mendelian randomization studies have not found a link between genetically determined differences in 25-OHD levels and cardiovascular endpoints [45-47]. In a recent very large Mendelian randomization study, there was an inverse relationship of vitamin D levels with all-cause mortality in people with 25-OHD levels <10 ng/mL; however, the associations with stroke and coronary heart disease were not statistically significant [48].
Vitamin D receptors are ubiquitous, with expression in many tissues; this explains the pleiotropic effects of vitamin D. Vitamin D receptor-deficient mice have increased renin expression, increased thrombogenesis, and more hypertension and cardiac hypertrophy than controls [49,50]. Chronic kidney disease patients are at risk of vitamin D deficiency, mainly driven by the decline in the activation of 25-OHD to 1,25-dihydroxyvitamin D. Fibroblast growth factor 23 (FGF23) levels are high in chronic kidney disease patients, and it was shown that this elevated level is associated with atherosclerosis and ventricular remodeling [51].
EVIDENCE FOR THE CARDIOVASCULAR EFFECTS OF CALCIUM WITH OR WITHOUT VITAMIN D SUPPLEMENTATION
Evidence from RCTs and observational studies
The controversies regarding cardiovascular safety of calcium and vitamin D replacement started with the WHI study. The study had a calcium/vitamin D arm where women with generally adequate calcium and vitamin D (including women taking supplements at baseline) were given additional calcium (1,000 mg) and vitamin D (400 IU) daily supplements or placebo. During 7 years of follow-up, neither MI/coronary heart disease, death, nor stroke showed differences between treatment groups (HR, 1.04; 95% CI, 0.92 to 1.18 and HR, 0.95; 95% CI, 0.82 to 1.10, respectively). Although this trial indicated a safe profile of calcium and vitamin D supplementation, it should be noted that the cardiovascular outcomes were prespecified as secondary outcomes (Table 1) [52]. The cardiovascular safety of calcium and vitamin D supplements was accepted until the work of Bolland et al. [53] in 2008 regarding a secondary analysis of an RCT where 1,471 postmenopausal New Zealand females, with a mean age of 74 years, were randomized to 1,000 mg of elemental calcium (without vitamin D) or placebo. Unlike the WHI trial, women taking calcium supplements at baseline were excluded. Although there was a statistically significant increase in the rate of self-reported MI in the calcium group compared to placebo (RR, 2.24; 95% CI, 1.20 to 4.17), the risk of angina, stroke, or the composite outcome (angina, chest pain, MI, or sudden death) was not significantly different between groups (Table 1). Moreover, an analysis of confirmed cardiovascular events attenuated the MI RR to 2.12 (95% CI, 1.01 to 4.47), and there was no significant difference in the composite endpoint of stroke, MI, and sudden death (RR, 1.47; 95% CI, 0.97 to 2.23) [53]. These study results have been challenged for a number of reasons. This was a secondary analysis of a study that was powered to detect bone density and fracture data, but not cardiovascular endpoints; there was a higher baseline risk for CV outcomes in patients assigned to the active calcium arm; and the results were inconsistent between the different cardiovascular outcomes [53]. These questions led Bolland et al. [54] to re-examine the WHI data according to baseline calcium and vitamin D supplementation. They hypothesized that calcium and vitamin D supplementation at baseline in the WHI study may have masked any potential cardiovascular risk of calcium supplementation [54]. Surprisingly, the data showed that in women not taking calcium supplements at baseline, the HR for cardiovascular events in subjects taking calcium and vitamin D supplements ranged from 1.13 to 1.22 (P=0.05 for clinical MI or stroke, P=0.04 for clinical MI or revascularization), while in women taking calcium supplements at baseline, the cardiovascular risk did not differ between treatment arms [54]. The gastrointestinal side effects of calcium supplementation can be mistaken by patients as symptoms of MI when this outcome is defined by patient self-reports; adjudication of cardiovascular events is therefore important [55]. To overcome this, Lewis et al. [56] conducted an RCT comparing calcium (1,200 mg daily) to placebo in 1,460 elderly women, with adjudicated cardiovascular endpoints. In that study, calcium supplementation was not associated with a higher risk of death or first-time hospitalization from atherosclerotic cardiovascular disease (HR,0.938; 95% CI, 0.690 to 1.275) (Table 1) [56]. In the long-term follow-up of the Randomized Evaluation of Calcium Or vitamin D (RECORD) trial, a subsequent randomized trial of calcium and vitamin D supplementation versus placebo, taking supplements was not associated with an increased risk of cardiac events (Table 1) [57]. More recent studies have also failed to demonstrate any increased cardiovascular risk in those taking calcium supplements. In 2013, Cauley et al. [58] reported the 5-year post-intervention outcomes of the WHI study. There were no significant differences in the risk of MI, stroke, and death between the calcium/vitamin D group and placebo. Interestingly, the same results were also seen when patients were examined according to their being on prior calcium at randomization or not [58]. Further safety data were reported from the UK biobank, a large prospective cohort including 475,255 participants (median age 58 years, 55.8% women). In a publication investigating the association between calcium and vitamin D supplementation and incident cardiovascular events including mortality, there was no association between calcium supplements and incident hospital admission for either ischemic heart disease or death [59]. In a large prospective cohort study of 132,823 participants followed for 17.5 years who consumed at baseline 1.5 to 1.7 dairy servings, higher all-cause mortality was observed in men who were taking ≥1,000 mg calcium supplements (RR, 1.17; 95% CI, 1.03 to 1.33) [60]. There was a dose-dependent inverse relationship between calcium supplementation and all-cause mortality in females for calcium intake of 0.1 to <500, 500–<1,000, and ≥1,000 mg/day, respectively (RR, 0.90; 95% CI, 0.87 to 0.94; RR, 0.84; 95% CI, 0.80 to 0.88; and RR, 0.93; 95% CI, 0.87 to 0.99). Interestingly, there was no association between dietary calcium and mortality in both males and females [60]. In a population-based, prospective cohort study of 34,468 patients with a median dietary calcium intake of 792 mg/day (interquartile range, 428 mg/day), calcium intake was not associated with higher cardiovascular death, MI, and stroke [61]. Several observational studies found that dietary calcium (total less than 1,500 mg) levels were not associated with cardiovascular disease endpoints [62,63]. An analysis of data from 35,983 women in the WHI study did not show a reduction in incident heart failure in the calcium and vitamin D group compared to placebo in the overall population (HR, 0.95; P=0.46) but a lower risk for heart failure in the low-risk group (patients without heart failure precursors at baseline, such as coronary artery disease, hypertension, and diabetes) (HR, 0.63, 95% CI, 0.46 to 0.87) [64]. Several other cohort studies reported conflicting results as to whether calcium supplementation can cause cardiovascular harm [65-73].
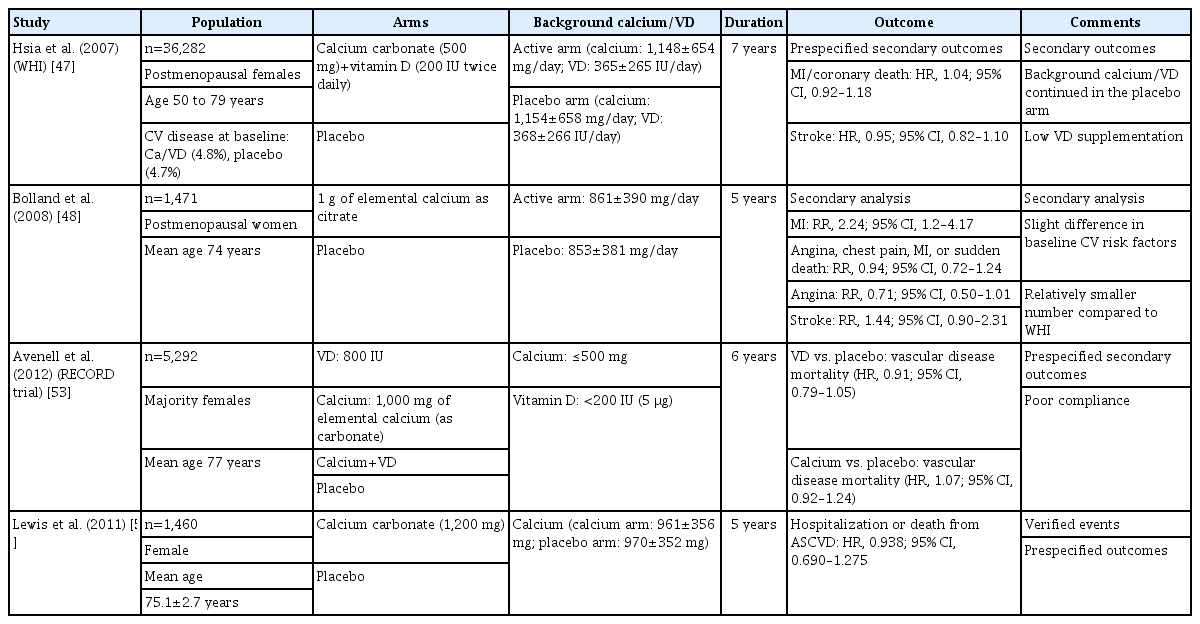
Important Trials of Calcium +/– Vitamin D on Cardiovascular Outcomes
Evidence from meta-analyses
Given the heterogeneity in the results of studies of calcium supplementation, Bolland et al. [74] in 2010 published a meta-analysis of the effect of calcium supplementation on cardiovascular outcomes. The trial-level analysis showed that calcium supplementation was associated with a higher risk of MI (RR, 1.27; 95% CI, 1.01 to 1.59), but not with stroke, composite endpoints, or death. Similarly, the patient-level analysis showed that the risk of MI increased by 31% in the group taking calcium (HR, 1.31; 95% CI, 1.02 to 1.67), with no significant differences in other cardiovascular outcomes [74]. This meta-analysis had multiple limitations, including the fact that cardiovascular outcomes were secondary outcomes, there was some self-reporting of outcomes, and there were differences in the administered calcium supplements [74]. In order to incorporate the WHI patients without baseline calcium supplementation in the meta-analysis, Bolland et al. [54] conducted another systematic review, including three RCTs. The pooled analysis showed again that calcium and vitamin D supplementation was associated with an increased risk of MI (RR, 1.21; P=0.04), stroke (RR, 1.2; P= 0.05), and the composite of MI or stroke (RR, 1.16; P=0.02) [54]. These data are limited by the heterogeneity of the studies and cardiovascular outcomes reported, the selection bias by including only the WHI patients not on baseline supplementation, and the fact that cardiovascular endpoints were secondary outcomes [54]. In 2013, a systematic review of calcium and vitamin D supplementation by Mao et al. [75] showed that calcium and vitamin D supplementation was not associated with a statistically significant difference in major cardiovascular events. In 2015, Lewis et al. [76] published a systematic review of 18 RCTs comparing calcium and vitamin D supplementation versus placebo. They found no significant differences in coronary heart disease hospitalization or death in five trials between calcium with or without vitamin D and control with a pooled RR of 1.02 (95% CI, 0.96 to 1.09; P=0.51). Pooled data from 17 trials showed no difference in all-cause mortality, with an RR of 0.96 (95% CI, 0.91 to 1.02; P=0.18). There were also no significant differences in the individual outcomes of MI, angina, and chronic coronary heart disease. A sensitivity analysis excluding patients in the WHI trial with baseline intake of calcium and vitamin D also showed no cardiovascular associations [76]. In 2016, a systematic review by Chung et al. [77] included clinical trials, prospective cohort studies, and case-control studies. This review again did not show a significant difference in cardiovascular events or mortality between calcium and vitamin D supplementation and placebo, although cardiovascular disease endpoints were secondary outcomes in all included trials [77]. A more recent systematic review in 2020 pooled 89,251 community-dwelling participants from RCTs examining the effect of calcium and vitamin D supplements compared to placebo. There was no significant difference in all-cause mortality between the experimental groups (calcium alone, vitamin D alone, or combination) and the control group. A pooled analysis showed that calcium supplementation was not associated with risk of MI and major adverse cardiovascular events [78].
Overall, there is no convincing evidence of cardiovascular harm from either dietary calcium or supplemental calcium (total up to 1,200 mg) and vitamin D.
EFFECT OF VITAMIN D ON CARDIOVASCULAR ENDPOINTS
Evidence from RCTs
Historically, the effect of vitamin D on cardiovascular outcomes was controversial and based mainly on studies where the primary endpoints were related to bone health [43]. In the last few years, three large RCTs have helped to answer the question of the cardiovascular effects of vitamin D supplementation. The Vitamin D Assessment Study (ViDA) was a 3.3-year randomized placebo-controlled trial investigating the effect of a vitamin D loading dose of 200,000 IU, followed by 100,000 IU monthly or placebo in 5,110 participants aged 50 to 84 years. The subjects had a mean serum 25-OHD of 25.3±9.5 ng/mL at baseline, and were recruited mostly from family practices in Auckland, New Zealand, with the primary outcomes of incident cardiovascular disease and death. The study showed no significant difference between vitamin D and placebo for all cardiovascular endpoints, with a combined HR of 1.02 (95% CI, 0.87 to 1.20) (Table 2) [79]. However, vitamin D-deficient individuals on vitamin D supplements demonstrated lower systolic blood pressure than controls (–7.5 mm Hg; 95% CI, –14.4 to –0.6 mm Hg; P=0.03) [80].
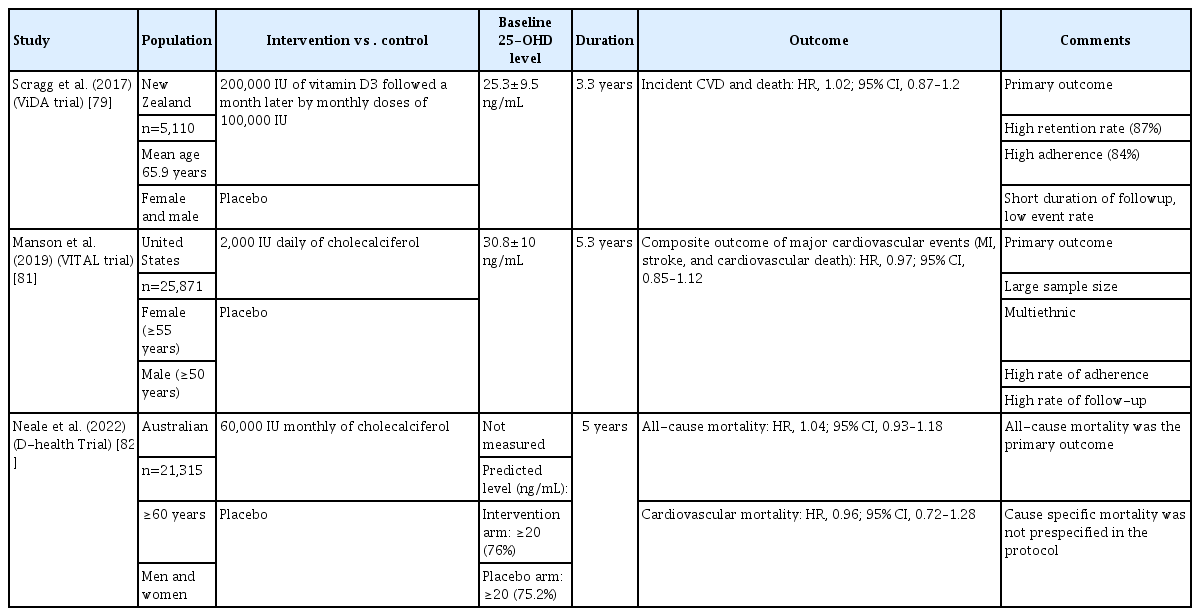
Important Trials of Vitamin D Supplementation on Cardiovascular Outcomes
The VITamin D and OmegA-3 TriaL (VITAL) trial was an RCT randomizing subjects to vitamin D3 (2,000 IU daily) over 5.3 years with a primary endpoint of cardiovascular events. The trial enrolled 25,871 subjects including men over 50 years and women over 55 years. There was no significant difference in composite major cardiovascular events (MI, stroke, and cardiovascular death) (HR, 0.97; 95% CI, 0.85 to 1.12) (Table 2) [81]. The D-Health trial was a randomized placebo-controlled trial of 21,315 participants over 60 years in Australia comparing 60,000 IU of vitamin D3 monthly to placebo for 5 years. This study showed no significant difference between vitamin D supplementation and placebo in the primary outcome of all-cause mortality and the secondary outcome of cardiovascular mortality (HR, 1.04; 95% CI, 0.93 to 1.18) and 0.96 (95% CI, 0.72 to 1.28) respectively. Serum 25-OHD was not measured as the hypothesis was to examine the potential benefit of vitamin D supplementation in the unscreened population. It is worth mentioning that all-cause mortality was the primary outcome and cause specific mortality was not prespecified in the protocol (Table 2) [82].
Evidence from meta-analyses
In a recent meta-analysis of 21 RCTs (including both the ViDA and VITAL trials, but not the D-Health trial) with over 83,000 patients mean age 65.8 years, vitamin D supplementation was not associated with a reduced risk of major adverse cardiovascular events (RR, 1.00; 95% CI, 0.95 to 1.06; P=0.85), individual cardiovascular endpoints (MI, stroke, or cardiovascular disease mortality), or all-cause mortality compared to placebo [83]. The result of these RCTs and a systematic review consistently showed the safety of modest doses of vitamin D supplementation, but a lack of cardiovascular benefits.
CALCIUM AND VITAMIN D SUPPLEMENTATION RECOMMENDATIONS FROM GUIDELINES
Various professional organizations have established calcium and vitamin D recommendations in their recent guidelines. The Bone Health and Osteoporosis Foundation (formerly the U.S. National Osteoporosis Foundation) recommends “a diet with adequate total calcium intake (1,000 mg/day for men aged 50 to 70 years; 1,200 mg/day for women ≥51 years and men ≥71 years), incorporating calcium supplements if intake is insufficient” [84]. The North American Menopause Society recommends that healthy postmenopausal females and those with osteoporosis should try to achieve a total daily calcium intake of 1,200 mg [85]. The Endocrine Society 2019 osteoporosis guidelines advise an intake of 1,000 to 1,200 mg of calcium from the diet if possible; supplements may be required in some individuals [14]. The American Association of Clinical Endocrinology 2020 osteoporosis guidelines recommend a total calcium intake of 1,200 mg daily including diet and supplements for women 50 years or older [86]. These recommendations are in line with the Institute of Medicine, which recommends 1,000 to 1,200 mg of calcium per day from diet and/or supplements [87]. In postmenopausal females and males over age 50 years at risk for fragility fractures or with osteoporosis, the National Osteoporosis Guidelines Group suggests a minimum intake of 700 mg of calcium, preferably from diet or otherwise from supplements. They recommend the consumption of vitamin D-rich food in addition to at least 800 IU of vitamin D supplements in patients with or at risk of vitamin D insufficiency. The same guidelines acknowledge that in order to achieve the target recommended intake, calcium and vitamin D supplementation is usually required in ambulatory and care facility patients [88]. It is recommended to screen for vitamin D deficiency and to guide vitamin D supplementation in high-risk patients (patients with chronic kidney disease, liver disease, malabsorption, osteoporosis, obesity, or pregnancy and patients on antiepileptic, antifungal, steroids, or cholestyramine) [32].
Professional society guidelines are consistent in their recommendations regarding the need for calcium and vitamin D nutrition, especially in the elderly and those with osteoporosis [14,84-88]. Although dietary calcium is preferred, they recognize the potential need for supplemental calcium to achieve calcium intake of 1,000 to 1,200 mg per day. The guidelines vary in their vitamin D recommended intake, ranging from 600 to 2,000 IU per day by supplements.
CONCLUSIONS
Although some randomized clinical trials and systematic reviews investigating the cardiovascular effects of calcium and vitamin D supplementation have suggested a risk of cardiovascular endpoints in patients on calcium supplements, the bulk of evidence does not support this. There is inconsistency across different cardiovascular endpoints, including mortality. Overall, there is a neutral effect of calcium and vitamin D supplementation on cardiovascular and mortality endpoints. Despite the importance of dietary calcium and vitamin D intake or supplementation to modest levels in order to maintain optimal bone health in elderly individuals, excessive calcium or vitamin D supplementation may have risks and has no additional benefit. Additional placebo-controlled clinical trials with primary cardiovascular endpoints involving calcium and vitamin D supplementation are unlikely due to ethical concerns. Therefore, with documented bone benefits and neutral cardiovascular concerns, modest calcium intake from the combination of diet and supplements, as well as supplemental vitamin D, should be recommended to our patients after middle age. The current guidelines largely support calcium intake of 1,000 to 1,200 mg, preferentially from diet, with supplements useful in patients unable to achieve adequate intake from dietary sources. Vitamin D supplementation from 800 to 2,000 IU daily would be prudent to maintain calcium homeostasis in older patients and especially those with osteoporosis or fracture risk. The current evidence does not support the use of calcium or vitamin D for the prevention of cardiovascular disease.
Notes
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.