Long-Term Outcomes Following Thermal Ablation of Benign Thyroid Nodules as an Alternative to Surgery: The Importance of Controlling Regrowth
Article information

Abstract
Thermal ablation (TA) procedures, such as radiofrequency ablation and laser ablation, are used for the treatment of benign thyroid nodules. Short-term studies (<2 years) have demonstrated that TA is an effective and safe procedure to improve cosmetic or symptomatic problems. However, studies including a longer follow-up period show that treated thyroid nodules can increase in size after 2 to 3 years. Several studies suggest that this results from regrowth at the undertreated nodule margins. Here, we review current data on regrowth after TA and describe factors related to it and possible approaches to prevent it.
INTRODUCTION
Thermal ablation (TA) procedures, such as radiofrequency ablation (RFA) and laser ablation (LA), are used to treat benign thyroid nodules [12]. Short-term studies (<1 to 2 years) showed that TA is effective and safe for the treatment of cosmetic or symptomatic problems, resulting in a reduction in nodule volume of 50% to 80% [2]. Some authors suggest that the primary purpose of TA is to improve pressure symptoms rather than to provide complete ablation [34]. When LA and RFA were first introduced in the 2000s, this paradigm formed the main strategy for patients who were either unable or unwilling to undergo surgery [56]. As an alternative to surgery, early TA was aimed at relatively short-term palliation due to the poor general condition of the patient when the initial volume of the nodule was relatively small. The goal of TA at that time was to achieve an approximately 50% volume reduction, generally over a 1-year period [3,4]. However, several studies with longer follow-up periods subsequently showed a tendency for the treated thyroid nodules to increase in size after 2 to 3 years [789]. With increasingly widespread awareness of the safety and effectiveness of TA, patients may choose minimally-invasive TA to avoid scarring in the highly-visible anterior neck area and to reduce the risk of hypothyroidism [10111213]. Therefore, to be considered as an alternative to surgery, TA procedures would need to be effective in the treatment of larger nodules and the effects of treatment should be sustainable for longer periods [91415]. With this goal in mind, we have reviewed the issue of regrowth in studies of TA and we describe the factors related to nodule regrowth and strategies to manage this problem.
DEFINITION AND FACTORS RELATED TO REGROWTH
To date, several TA studies have reported unsatisfactory results related to regrowth and/or the need for further treatment, such as additional TA or surgery (Table 1) [791516,171819,2021]. In their 2009 study of RFA for the treatment of autonomous nodules, Baek et al. [22] reported observations of regrowth of the untreated peripheral regions, and later described this as ‘marginal regrowth’ [8]. However, similar terms, such as regrowth, marginal regrowth, and recurrence are used under different definitions and criteria. Some researchers prefer to use the term ‘recurrence’ while others prefer to use ‘regrowth’ under virtually the same meaning [2324]. Many authors have defined regrowth as an increase in nodule volume >50% over the previously recorded volume [7925]. Others define regrowth as a post-treatment volume greater than the initial nodule volume [16]. Papini et al. [17] used the term ‘partial regrowth’ when the volume was >20% larger than the volume at 1 year after treatment. Authors have also applied the term regrowth to indicate an increase in nodule volume, but without providing quantitative criteria [26].
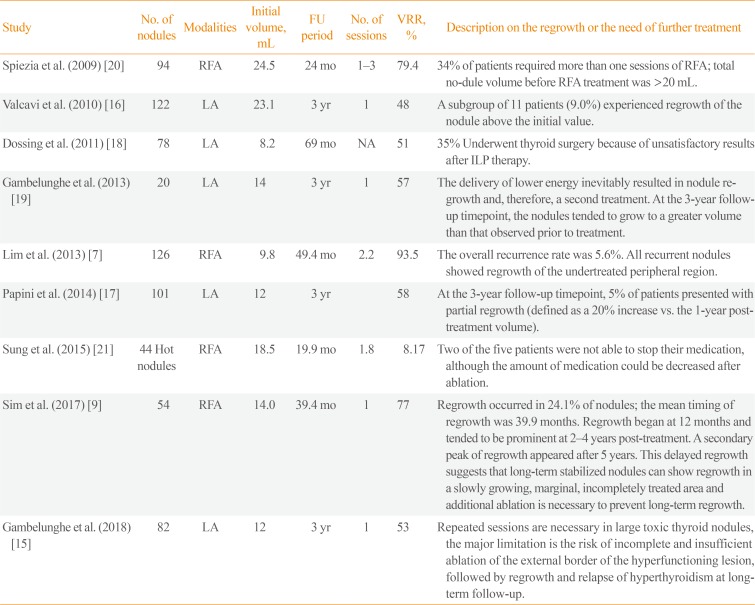
Studies Referring to Nodule Regrowth or a Requirement for Multiple Sessions of Thermal Ablation
For this manuscript, we defined nodule regrowth as an increase of >50% over the smallest previously recorded volume. Marginal regrowth is used to describe the phenomenon of regrowth occurring from the undertreated peripheral areas. Most cases of regrowth occur as a result of marginal regrowth.
If the margin of the nodule is insufficiently ablated, regrowth can occur sometime after TA; one 4-year follow-up study reported that solid nodules tended to regrow after 2 years [7]. A follow-up study of up to 7 years after single-session ablation reported that regrowth occurs in 24.1% of cases, at an average of 39 months after RFA [9].
The most common risk factor for marginal regrowth is a large initial nodule volume [1827]. In a study by Wang et al. [24], 16 of 110 patients experienced recurrence 12 months after microwave ablation and the mean initial volume of the nodules showing recurrence was significantly larger than the non-recurring nodules. The ablation technique is considered to be another important factor associated with regrowth. Lim et al. [7] described regrowth occurring from the incompletely-treated peripheral regions and concluded that controlling the peripheral margin of the nodule with a moving-shot technique is important to prevent marginal regrowth. The anatomical location of the nodule should also be considered. Nodules that are too close to critical structures, such as the recurrent laryngeal nerve or carotid sheath, are more likely to undergo regrowth from the viable tissue remaining after incomplete ablation [2829].
ADEQUATE APPLICATION OF MULTIPLE SESSION ABLATION
According to the 2017 thyroid RFA guidelines developed by the Korean Society of Thyroid Radiology, multiple-session ablation may be required for large nodules [1], and this view has been supported by other authors [1930]. However, there is no consensus about the specific indication or appropriate timing for multiple ablations [2].
Cervelli et al. [31] noted that in nodules with a post-treatment volume >9 mL and a residual viable tissue volume >4 mL, additional ablation should be performed 1 year after treatment when the ablated tissue has become sufficiently fibrotic. They suggested that during the 1-year post-treatment period, the ablated tissues, which are mainly located at the center of the nodule, are absorbed and the marginal residual tissue is at a sufficient thickness to be treated by additional ablation [31]. Huh et al. [30] compared the outcomes between patients undergoing single-session RFA and those receiving additional ablation 1 month later, showing no significant difference in the 1-year follow-up results between the two groups. The lack of effect in Huh's study [30] may be due to the relatively small size of treated nodules and short interval between the first RFA and the additional ablation. At 1-month post-treatment, residual marginal tissue would be thin and additional ablation may, therefore, not be effective.
Recent studies have focused on the need for earlier identification of nodule regrowth. Sim et al. [9] proposed a method of tracking the volume of the nodule after RFA by dividing it into the total volume (Vt), ablated volume (Va), and viable volume (Vv). Because the reduction in Va occurs rapidly in the initial stages after RFA, growth of the Vv may be masked and Vt may be misinterpreted as decreasing. Therefore, measuring the Vv separately is advantageous for identifying earlier signs of regrowth (Fig. 1) [9]. While very few studies have provided evidence for the appropriate timing for additional ablation, assessment of the Va, Vv, and Vt during follow-up can provide a useful indication. When the Vv begins to increase, it is time to consider additional ablation; when the Vv increases and the Va is small, as shown in Fig. 1C, it is an appropriate point to perform additional RFA. However, even if the Vv is increasing, if the Va is rapidly decreasing, it is advisable to delay additional ablation, and ultrasonography follow-up at 1- to 3-month intervals should be conducted. When the rate of increasing Vv exceeds the rate of decreasing Va, additional ablation should be considered.
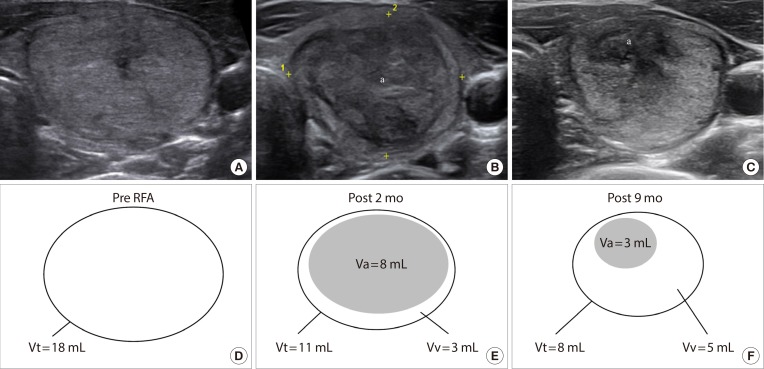
Ultrasonography of a thyroid nodule: (A) pre-radiofrequency ablation (RFA), (B) 2 months post-RFA, and (C) 9 months post-RFA. (D-F) Diagrams indicate the total volume (Vt), ablated volume (Va), and viable volume (Vv) at these timepoints. Although Vt decreases over time, Vv increased by 2 mL between months 2 and 9, indicating that growth of the residual viable nodule tissue had already begun. In this case, additional RFA was performed 1 month after obtaining the image in C. aThe centrally-located hypoechoic area of ablated tissue is indicated.
Other efforts have been made to identify the remaining viable portion of nodules through contrast-enhanced ultrasonography (CEUS). CEUS can be used to detect the undertreated area immediately or shortly (1 month) after TA, enabling prompt delivery of additional treatment [27,32,33,34]. This method is one approach to increasing the ablation ratio, as described in the section below [34].
ADVANCES IN TECHNIQUES FOR REDUCING MARGINAL REGROWTH
When the volume of a nodule is too large to completely ablate it in single session of TA, the initial session aims to ablate the nodule tissue as much as possible. The extent of ablation within the Vt, i.e., the ablation ratio, has a significant impact on future volume reduction. Recently, Sim et al. [35] used the term initial ablation ratio (IAR). Ablation ratio is a ratio of the volume of ablated tissue to the total nodule volume. IAR is an ablation ratio calculated shortly after TA. The meaning of IAR is how much did an operator ablate the nodule tissue with TA. Thus, IAR is a quantitative index representing the performance of a TA procedure, in other words, how well an operator did the TA. In their study, they found that the IAR and the volume reduction ratio (VRR) were positively correlated, so that a high VRR was achieved when IAR was high, and 50% VRR could be expected when ≥70% IAR was achieved [35]. Gambelunghe et al. [19] suggested that complete ablation (or a very high percentage of ablation) is essential to achieve a marked reduction in the thyroid nodule. In a high intensity focused ultrasound study of mild Graves' disease, Lang et al. [36] hypothesized that the ablation volume ratio may be a factor in disease relapse.
By contrast, once the volume of the nodule has reduced, it is important to minimize the amount of residual tissue in order to limit regrowth. To achieve this, different techniques and devices are required. Vascular ablation techniques were recently introduced by Park et al. [37], namely, the artery-first ablation technique and the marginal venous ablation technique. The artery-first technique ablates the tumor-feeding artery first to minimize the heat-sink effect and to reduce the possibility of hemorrhage during the procedure. The draining vein, which is primarily located in the margin of the tumor, interferes with the complete ablation of the margin due to the heat-sink effect. Ablation of these veins can lead to complete ablation of the nodule margin. After puncturing a portion of the vein with the electrode, ablation is initiated when air bubbles are formed and flow into the veins. While this occurs, the veins are filled with hot air bubbles and venous flow eventually ceases, retaining white air bubbles in the lumen of the marginal veins. The marginal venous ablation technique is particularly helpful to prevent marginal regrowth (Fig. 2) [37].
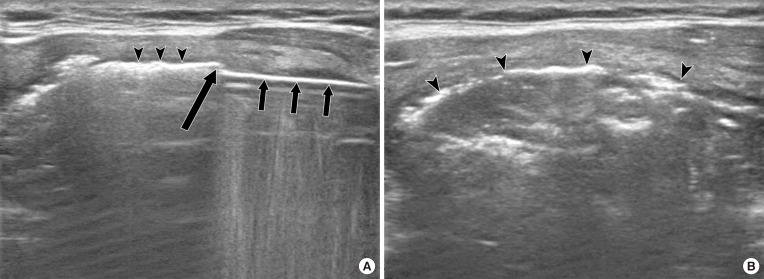
(A) An electrode (short arrows) directly ablates the perinodular vein (arrow). Air bubbles are seen inside the venous lumen (arrowheads). (B) After completing venous ablation, compact filling of hot air bubbles is observed (arrowheads).
When the nodule tissue is close to a critical structure, it is technically difficult to ablate the tissue completely. This situation is common on the medial side, near the recurrent laryngeal nerve, around the carotid sheath where the vagus nerve and sympathetic ganglions are located, and on the posterior side, where anatomical variation occasionally occurs [29]. Therefore, it is helpful to artificially create a margin of safety at these locations. The hydrodissection technique is one method used for this purpose and involves the injection of a fluid, such as 5% dextrose [1]. After the needle is inserted between the nodule and the critical structures, ablation is performed while fluid is continuously injected, or immediately after injecting fluid to form safety margin of ≥5 mm. Using this method, effective ablation can be achieved, thereby minimizing the residual margin of viable tissue [3237].
CONCLUSIONS
With greater knowledge of the factors associated with nodule regrowth and strategies to manage this issue, it is possible to improve the clinical outcome of TA by minimizing marginal regrowth. In so doing, it is possible that the outcomes of TA may be comparable to that of surgery.
Notes
CONFLICTS OF INTEREST: This study received no funding in the form of grants. Jung Hwan Baek's financial activities are not related to the present article (patent holder of a unidirectional ablation electrode); he has been a consultant to two radiofrequency companies, STARmed and RF Medical, since 2017.