Recent Topics in Fibrodysplasia Ossificans Progressiva
Article information

Abstract
Fibrodysplasia ossificans progressiva (FOP) is a rare genetic disease that is characterized by the formation of heterotopic bone tissues in soft tissues, such as skeletal muscle, ligament, and tendon. It is difficult to remove such heterotopic bones via internal medicine or invasive procedures. The identification of activin A receptor, type I (ACVR1)/ALK2 gene mutations associated with FOP has allowed the genetic diagnosis of FOP. The ACVR1/ALK2 gene encodes the ALK2 protein, which is a transmembrane kinase receptor in the transforming growth factor-β family. The relevant mutations activate intracellular signaling in vitro and induce heterotopic bone formation in vivo. Activin A is a potential ligand that activates mutant ALK2 but not wild-type ALK2. Various types of small chemical and biological inhibitors of ALK2 signaling have been developed to establish treatments for FOP. Some of these are in clinical trials in patients with FOP.
INTRODUCTION
Fibrodysplasia ossificans progressiva (FOP) (OMIM #135100) is a rare genetic disease that is characterized by the formation of heterotopic hard tissues in soft tissues, such as skeletal muscle, ligaments, and tendons [123]. FOP is an autosomal dominant disorder with an incidence of approximately one patient per 2 million people worldwide regardless of race, location, or gender [12]. The hard tissue formed in affected patients is not simply mineralized calcium phosphate but represents the formation of new bone tissue by osteoblasts through a cartilaginous template (endochondral ossification) via the same process that is observed in normal skeletal tissues during embryonic development and regeneration. Moreover, the heterotopic bone tissue contains bone marrow and is metabolized by osteoclasts and osteoblasts in a manner similar to that observed in normal bone tissues. Heterotopic bones are distinguishable from normal bone tissues by their locations but not their biochemical characteristics, and it is therefore hard to remove only the heterotopic bone tissues in internal medicine procedure performed in patients with FOP. Although most patients with FOP can move their joints normally at birth, they show disability in various joints, including the jaw, once they reach their 30's because the heterotopic bones that formed in skeletal muscle, tendons, and ligaments gradually fuse with each other and bridge with normal bones, fixing the joints [4]. Moreover, injury to soft tissues causes acute heterotopic bone formation in patients with FOP. Thus, invasive procedures, such as biopsy, surgical operation, and injection, are prohibited in patients with FOP [5].
Achieving a diagnosis of FOP before the onset of heterotopic ossification was difficult for a long time because there were no reliable biomarkers for this disease that could be evaluated in peripheral blood or urine. Moreover, the molecular mechanisms underlying the pathogenesis observed in patients with FOP were unknown because tissue samples were not accessible due to the contraindication for invasive procedures. The identification of the activin A receptor, type I (ACVR1)/ALK2 gene in 2006 as a gene that is responsible for FOP was a breakthrough for this rare disease [6]. The ACVR1/ALK2 gene encodes a transmembrane kinase receptor, ALK2, that binds bone morphogenetic proteins (BMPs). BMP was originally found in 1965 and described as a unique molecule in the bone matrix that induces heterotopic bone to develop in skeletal muscle [7]. The identification of a recurrent heterozygous mutation in the ACVR1/ALK2 gene in sporadic and inherited cases of FOP directly connected the BMP and FOP research fields. Moreover, those findings allowed us to examine the molecular mechanism underlying heterotopic ossification both in vitro and in vivo, to improve the diagnosis of the disease and search for potential therapeutic molecules for FOP in cultured cells and experimental animals. Because ALK2 is associated with FOP as a gain-of-function mutant receptor, various types of inhibitors have been developed to establish therapeutic drugs for FOP. Some of these molecules are in phase 2 or 3 clinical trials of patients with FOP. In this article, we review the basics of potential therapeutics for the rare disease FOP.
CLINICAL FEATURES OF FOP
The most typical clinical feature of FOP is progressive heterotopic bone formation in soft tissues that causes disability in the joints. The progression of disability in FOP patients follows some patterns: from the upper to lower, proximal to distal and dorsal to ventral side (Table 1) [8]. The neck, spine and shoulder are the most frequently affected sites (more than 80% of cases observed until patients younger than 15 years old) [5]. In contrast, the wrists and ankles are affected in approximately 50% of patients over 30 years old. The elbows, knees, hips, and jaw become gradually affected with age until the patient reaches 40 years old. Heterotopic ossification starts in childhood and continues through adulthood but is not observed at birth. However, lumbar puncture and surgical intervention induced acute heterotopic bone formation in a 10-week-old boy [9], suggesting that co-operation between a genetic mutation and an inflammatory environment induces heterotopic bone formation in patients with FOP.

Major Features of Patients with Fibrodysplasia Ossificans Progressiva
One of the clinical features detectable at birth, before the onset of heterotopic ossification, is malformations in the big toes (Table 1). More than 90% of patients who have FOP show such malformations [51011]. An additional typical feature observed in FOP patients is tumor-like swellings [11]. Flare-ups are frequently observed before the formation of heterotopic bones is observed in soft tissues [12]. Therefore, if a patient shows both of these clinical features (malformation of the big toes and swelling), FOP should be considered before invasive procedures are performed. However, some patients with FOP do not show any clinical features before the onset of heterotopic ossification.
DIAGNOSIS OF FOP
More than 90% of patients with typical FOP have an identical genetic mutation consisting of a guanine to adenine change at position 617 (c.617G>A) in the ACVR1/ALK2 gene. This causes a substitution mutation in the ALK2 protein: Arg to His at position 206 (p.R206H) (Fig. 1). Additional mutations that occur at different positions in the ACVR1/ALK2 gene have also been identified in patients with FOP with different clinical features (Fig. 1). Although some other genes were suggested to be related to FOP before the identification of the ACVR1/ALK2 gene in 2006 [6131415], no case of FOP has been shown to carry a mutation in a gene other than ACVR1/ALK2, suggesting that FOP is a typical monogenic disorder. The ACVR1/ALK2 gene is located on chromosome 2 in humans and consists of 9 coding exons. It encodes the ALK2 protein, which is a transmembrane serine/threonine (Ser/Thr) kinase receptor for members of the transforming growth factor-β (TGF-β) family (Fig. 1). Today, FOP is diagnosed by analyzing genetic mutations in the ACVR1/ALK2 gene by Sanger sequencing of polymerase chain reaction products obtained by amplifying each coding exon. Interestingly, all of the mutations identified in patients with FOP have been localized in exons 4 through 7, which encode the intracellular functional domains, the glycine/serine-rich (GS) and Ser/Thr kinase domains, both of which are important for intracellular signaling in response to ligand binding at the extracellular domain (Figs. 1, 2).

Schematic representation of the relationship between the activin A receptor, type I (ACVR1)/ALK2 gene, complementary DNA (cDNA) and protein. The ACVR1/ALK2 gene consist of 9 coding exons (Ex.) (black boxes). The ACVR1/ALK2 cDNA (1,530 bp) encodes a protein with 509 amino acids (a. a.). Mutations associated with fibrodysplasia ossificans progressiva are shown in the figure. The positions of the mutations in the cDNA and protein are indicated by numbers that begin from the adenine of the first ATG codon and Met residue, respectively. TGA, stop codon; SP, signal peptide; TM, transmembrane domain; GS, glycine/serine-rich domain; Ser/Thr kinase, serine/threonine kinase domain.
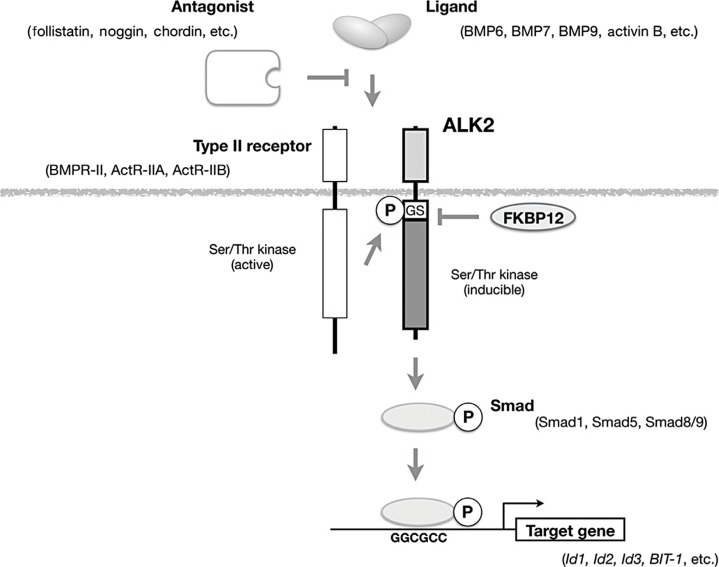
Schematic representation of signal transduction by ALK2 in response to ligand binding. ALK2 binds to a transforming growth factor-β family ligand, such as bone morphogenetic protein 6 (BMP6), BMP7, and BMP9, and acts as a type I receptor in co-operation with one of the type II receptors (BMP receptor type II [BMPR-II], activin receptor type IIA [ActR-IIA], and activin receptor type IIB [ActR-IIB]). Antagonists, such as follistatin, noggin, and chordin, directly bind to the ligand and prevent it from binding to receptors. Type II receptors are constitutively active kinases that phosphorylate the glycine/serine-rich domain (GS) domain of ALK2 to activate kinase activity. Activated ALK2 phosphorylates downstream substrates, such as Smad1, Smad5, and Smad8/9, and then binds to specific DNA sequences to regulate the transcription of its target genes. Ser/Thr, serine/threonine; P, phosphorylation; FKBP12, 12 kDa FK506-binding protein; Id1, inhibitor of DNA binding 1; BIT-1, BMP-inducible transcript-1.
MOLECULAR MECHANISMS OF PATHOGENESIS IN FOP
The extracellular domain of ALK2 (a type I receptor) binds to several ligands in the TGF-β family, such as BMP-6, BMP-7, BMP9, and activin B, in co-operation with type II receptors, such as BMP receptor type II (BMPR-II), activin receptor type IIA (ActR-IIA), and activin receptor type IIB (ActR-IIB) (Fig. 2). Because type II receptors are constitutively active Ser/Thr kinases, ALK2 is phosphorylated in a ternary complex formed in response to ligand binding at the cell membrane (Fig. 2). The GS domain, which is a stretch consisting of glycine and serine residues, has been identified as the site of phosphorylation by type II receptors [16]. Phosphorylated ALK2 activates kinase activity and phosphorylates Ser and Thr residues in downstream substrates, such as Smad1, Smad5, and Smad8/9 [171819]. Phosphorylated Smad proteins regulate the transcription of target genes in the nucleus [2021].
Transient over-expression of the mutant ALK2 associated with FOP, but not of wild-type ALK2, activates intracellular signaling without adding exogenous ligands, suggesting that these are gain-of-function mutations [22232425]. The mutant ALK2 associated with FOP is hypersensitive to the kinase activity of the type II receptors [25]. The 12 kDa FK506-binding protein (FKBP12) acts as a repressor of the kinase activity of type I receptors in the TGF-β family, including ALK2, by binding to their unphosphorylated intracellular domains [26]. It has been proposed that mutations in the intracellular domains of ALK2 associated with FOP reduce binding affinity to FKBP12 and activate downstream intracellular signaling in patients. Co-expression of the mutant ALK2 and FKBP12 in vitro reduced intracellular signaling by ALK2, but one of the mutant ALK2 associated with FOP, delP197_F198insL, was resistant to suppression by FKBP12 because it has lost the site at which it interacts with FKBP12 [27]. The clinical features of a patient carrying the mutation delP197_F198insL seemed to be similar to and not more severe than those observed in patients with typical FOP [2829]. All mutations in ALK2, including the delP197_F198insL mutation, are activated by co-expression with type II receptors, suggesting that the heterotopic ossification observed in patients is induced by intracellular signaling through mutant ALK2 in co-operation with type II receptors [2527].
A knock-in mouse model of the p.R206H mutation showed that the phenotypes were similar to those of patients with FOP, such as malformations of the fingers and heterotopic ossification. However, they were lethal after birth [30]. A conditional knock-in mouse model with the same mutation also showed heterotopic ossification after the induction of mutant ALK2 expression [31]. In the conditional knock-in mice, heterotopic ossification was blocked by trea tment with dominant negative type II receptors, suggesting that heterotopic ossification is a ligand-dependent event [31]. Activin A is a potential ligand for heterotopic bone formation in patients with FOP because the ALK2 mutant p.R206H but not wild-type ALK2 activated intracellular signaling in response to activin A, which is not TGF-β family osteogenic ligand [3132].
Sources of the chondrocytes and osteoblasts in heterotopic ossification were studied in vivo via a lineage tracing technique in several transgenic mouse models. Both chondrocytes and osteoblasts were differentiated from progenitor cells positive for Tie-2, a typical marker of endothelial cells [33]. Indeed, human endothelial cells underwent endothelial-mesenchyme transition following the over-expression of the p.R206H mutant of ALK2 or treatment with BMP or TGF-β in vitro [34]. During BMP-induced heterotopic bone formation in skeletal muscle tissue, both chondrocytes and osteoblasts were differentiated from Sca-1-positive interstitial mesenchymal cells but not myogenic lineage or endothelial cells [35]. Similarly, fibro/adipogenic mesenchymal cells and tendon-associated cells were identified as two types of progenitors for heterotopic ossification in an FOP mouse model that carried a mutant form of ALK2 [3637].
DEVELOPMENT OF NOVEL TREATMENTS FOR FOP
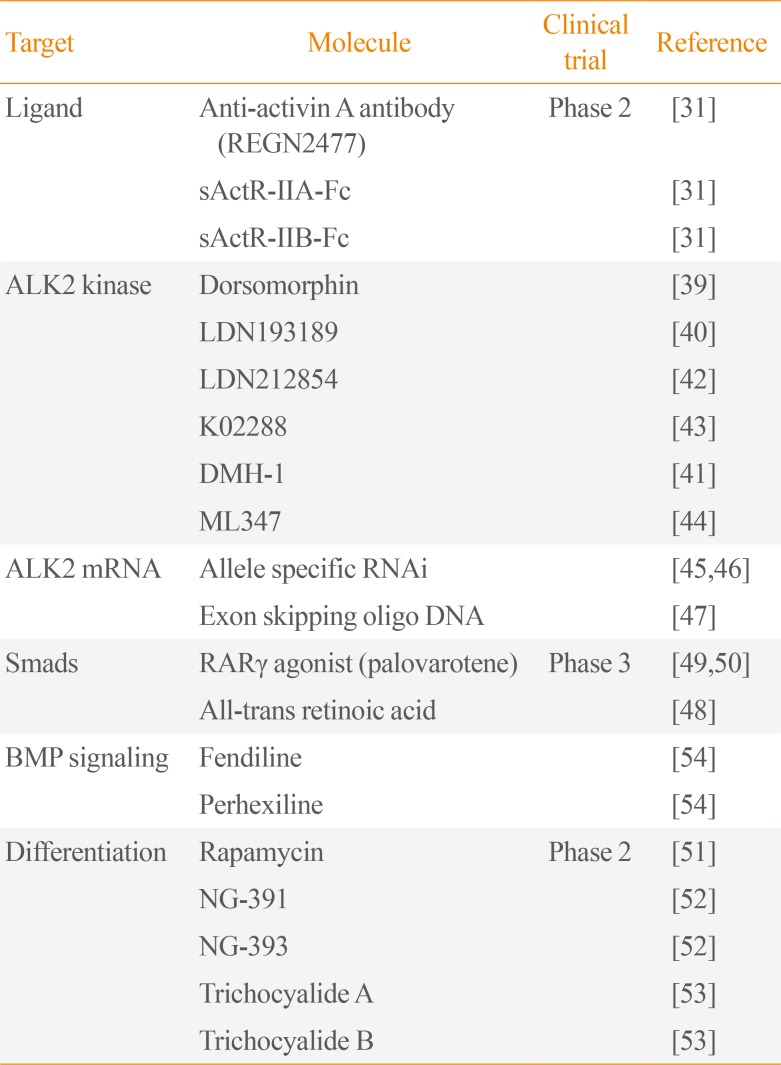
Because ALK2 over-signaling seemed to induce heterotopic ossification in FOP, various types of small chemical and biological inhibitors of ALK2 itself or of the up/down-stream factors in its intracellular signaling pathway have been explored (Table 2). A human anti-activin A-neutralizing antibody (REGN2477) was shown to inhibit heterotopic ossification in a mouse model with a conditional knock-in of p.R206H [31]. Using this antibody, the expansion of heterotopic ossification was also shown to be an activin A-dependent event [38]. Currently, the human anti-activin A antibody (REGN2477) is in a phase 2 clinical trial.

Inhibitors of ALK2 Signaling
Many small chemical compounds target the Ser/Thr kinase activity of ALK2. Dorsomorphin is the original compound found to act as a kinase inhibitor of type I receptors in the BMP subfamily [39]. LDN193189 was the earliest compound shown to inhibit heterotopic ossification in vivo in a mouse model of FOP [40]. Several additional kinase inhibitors have been developed to increase specificity for ALK2 among type I receptors [41424344]. However, no such compounds are currently in clinical trials.
Some nucleic acid-based therapies have been examined in FOP. RNA interference techniques were developed to inhibit mutant but not wild-type ALK2 [4546]. An additional single nucleotide mismatch to the FOP-causing mutation increased the specificity of the mutant alleles in both the p.R206H and p.G356D mutations [45]. Exon-skipping oligo DNA was also reported to remove mutant ALK2 proteins [47].
Chondrogenesis is inhibited by all-trans retinoic acid (RA), especially via RA receptor γ (RARγ) [48]. RARγ agonists, including palovarotene, have been shown to inhibit BMP signaling by reducing steady-state levels of Smad proteins and inhibiting heterotopic ossification in mouse models of transplantation of BMP ligands or that express mutant ALK2 in vivo [4950]. Palovarotene is currently in a phase 3 clinical trial.
Inhibitors of BMP signaling that act through mutant ALK2 have been screened in various in vitro models. Several mammalian target of rapamycin (mTOR) inhibitors, including rapamycin, were found to be inhibitors of chondrogenesis in induced pluripotent stem (iPS) cells derived from patients with FOP who carried the p.R206H mutation [3251]. Rapamycin has been approved for and is used in other diseases, and a phase 2 clinical trial for FOP has been started. Several small chemical inhibitors of in vitro mutant ALK2 p.R206H-induced osteoblastic differentiation in C2C12 myoblasts have been reported [5253545556].
CONCLUSIONS
In patients with FOP, heterotopic ossification is caused by gain-of-function mutations in the intracellular domains of ALK2, a type I receptor for osteogenic BMPs. The mutant ALK2 still requires ligand stimulation to induce heterotopic ossification. Various types of inhibitors of ALK2 have been studied with the aim of developing potentially effective treatments for heterotopic ossification in FOP. Some small chemicals and biological inhibitors are currently in clinical trials in patients with FOP.
ACKNOWLEDGMENTS
We would like to thank the members of the Division of Pathophysiology, Research Center for Genomic Medicine, Saitama Medical University and the Project of Clinical and Basic Research for FOP, Saitama Medical University for valuable discussions. Takenobu Katagiri would also like to thank Dr. Sang Wan Kim of Seoul National University College of Medicine, Korea for generously inviting us to write this review article. This work was supported in part by grants-in aid from the Ministry of Education, Culture, Sports, Science and Technology (MEXT) of Japan (17H04317 to TK and 17K11026 to ST), a grant-in-aid from the Japan Agency for Medical Research and Development (AMED) under grant number JP17pc0101007 to Takenobu Katagiri, and a Maruki Memorial Award of Saitama Medical University to Takenobu Katagiri (No. 17-A-1-01).
Notes
CONFLICTS OF INTEREST: Takenobu Katagiri received research grants from Daiichi-Sankyo, Co. Ltd. Sho Tsukamoto, Yutaka Nakachi, and Mai Kuratani do not have potential conflicts of interest relevant to this article.