Radiographic Characteristics of Adrenal Masses in Oncologic Patients
Article information

Abstract
Background
We aimed to assess the usefulness of pre-contrast Hounsfield unit (HU) and mass size on computed tomography to differentiate adrenal mass found incidentally in oncologic patients.
Methods
From 2000 to 2012, 131 oncologic patients with adrenal incidentaloma were reviewed retrospectively. Receiver operating characteristic (ROC) curves were applied to determine the optimal cut-off value of the mean HU and size for detecting adrenal metastasis.
Results
The median age was 18 years, and 80 patients were male. The initial mass size was 18 mm, and 71 (54.2%) of these were on the left side. A bilateral adrenal mass was found in 11 patients (8.4%). Biochemically functional masses were observed in 9.2% of patients. Thirty-six out of 119 patients with nonfunctional masses underwent adrenalectomy, which revealed metastasis in 13. The primary cancers were lung cancer (n=4), renal cell carcinoma (n=2), lymphoma (n=2), hepatocellular carcinoma (n=2), breast cancer (n=1), and others (n=2). The area under the curve for the size and HU for clinically suspicious metastasis were 0.839 (95% confidence interval [CI], 0.761 to 0.900; P<0.001) and 0.959 (95% CI, 0.898 to 0.988; P<0.001), respectively. The cut-off value to distinguish between metastasis and benign masses were 22 mm for size and 20 for HU.
Conclusion
ROC curve results suggest that pre-contrast HU >20 can be used as a diagnostic reference to suggest metastasis in oncologic patients with adrenal masses.
INTRODUCTION
In any patient with a history of cancer, the discovery of adrenal mass requires appropriate diagnostic approaches. Previous studies showed that most of the adrenal incidentalomas (AIs) are benign; however, 2.5% of these cases were metastases to the adrenal gland from another cancers [1]. Most of these results have been suggested in the studies of non-oncologic patients. Furthermore, incidence of incidental metastases was reported to be very low, since these studies excluded patients with known malignancy. Clinical implication of adrenal masses detected in oncologic patients should be distinct from non-oncologic patients. The adrenal gland is a relatively frequent site for metastases in patients with known extra-adrenal cancer. As many as 30% to 40% of lung cancers and 20% to 30% of breast cancers have adrenal metastases [23]. When adrenal masses are detected in cancer patients, it is critical to differentiate between benign adrenal adenoma and metastasis for treatment planning and prediction of prognosis. Patients with adrenal metastases are typically asymptomatic, and the incidence of Addison's disease in a clinical setting is very low. Therefore, imaging diagnosis is crucial for the evaluation of adrenal mass in patients with extra-adrenal cancer. Most cases of AI are often detected on abdominal computed tomography (CT), which is normally performed for reasons other than adrenal diseases. For AI in non-oncologic patients, the tumor size, washout of contrast dye, and noncontrast CT attenuation values expressed in Hounsfield units (HU) are used for distinguishing between benign and malignant adrenal masses [145]. For these patients, common radiographic features of malignant adrenal masses on the CT include a tumor size greater than 4 cm, irregular borders, heterogeneous enhancement, and lesions that demonstrate <40% of the relative percentage washout (RPW) or <60% of the absolute percentage washout (APW) [567].
In previous studies, a cut-off value <10 HU of an adrenal mass increased the likelihood of adenoma sensitivity, and specificity by 71% and 98%, respectively [8]. There are few studies on the radiographic features of AI in patients with extra-adrenal cancer.
In this study, we assessed the usefulness of pre-contrast HU and size of the tumor on CT to differentiate between a benign and malignant adrenal tumor in patients with extra-adrenal cancer.
METHODS
Institutional Review Board of Seoul National University Hospital approved this retrospective study (#1506-047-679). This study was conducted with AI patients who had been diagnosed previously or concurrently with cancer at the age 18 years or older. Subjects who had clinical symptoms of adrenal disease were excluded.
A total of 156 subjects underwent radiographic and endocrinologic evaluation at our hospital from January 2000 to December 2012. Data were collected from the medical records of patients included the patient's age, sex, presence of distant metastasis, and pathologic reports of adrenal mass after adrenalectomy or fine needle aspiration biopsies. The size, location, and characteristics of all adrenal masses were examined on CT, and the CT findings were based on reports of our radiologists. The pre-contrast HU measurement was obtained in 82.4% of adrenal masses. A circular region of interest was placed over the adrenal mass, and the mean attenuation value was recorded. The longest diameter of the adrenal mass was measured on an image showing the maximal cross-sectional area.
Functional studies were performed included a 24-hour urinary metanephrine, catecholamine, and serum cortisol test, as well as a 24-hour urinary cortisol and overnight 1 mg dexamethasone suppression test (DST). If hypertension was present, the plasma aldosterone concentration and plasma renin activity were measured. Pheochromocytoma was defined as AI with elevated urinary metanephrine and catecholamine levels compared to the reference. A plasma aldosterone/renin ratio of ≥20 was highly suggestive of primary aldosteronism. The saline load test was performed for diagnosis in four out of six patients. The subjects were diagnosed with subclinical Cushing syndrome if the post-overnight DST 8:00 AM serum cortisol level remained above 5 mcg/dL. Subjects with functional tumors, tumors >4 cm, and lesions suspected of being malignant on imaging underwent adrenalectomy, or this technique was performed concurrently with their surgery for primary cancer.
All the masses were categorized as clinically suspicious benign tumors or metastases. To distinguish between benign and malignant tumors, pathologic diagnosis, CT findings, oncologists' opinion, uptake value on [18F]-fluorodeoxyglucose (FDG) positron emission tomography-CT, and reports of magnetic resonance imaging were also included. A lesion was considered malignant if it showed a significant increase or decrease in size over a short period of time. If there was no change in the size for at least 12 months or longer without any cancer treatment, it was defined as clinically suspicious benign tumor. Sixteen subjects were excluded because they had not undergone either a pathological examination or a follow-up CT imaging for at least 12 months. Nine out of 140 subjects with distant metastasis were categorized as indeterminate to differentiate between benign and metastasis. Finally, this study included 131 subjects, and 26 masses were categorized as clinically suspicious metastasis, out of which increased FDG uptake was observed in 20 masses.
Statistical analyses were performed with SPSS version 21.0 (IBM Co., Armonk, NY, USA). The variables were expressed as median and in the interquartile range or as numbers with a percentage. The groups were compared using the Mann-Whitney U test for continuous variables. Receiver operating characteristic (ROC) curve analysis was used to suggest the reference for the size and mean HU for malignant adrenal masses. We compared the area under the curve (AUC) of HU, size, and combination of the HU and size through the pairwise comparison of ROC curves using statistical software, Medcalc (Medcalc, Ostend, Belgium). Statistical significance was indicated as P<0.05 for all tests.
RESULTS
Clinical characteristics of the subjects
A total of 131 oncologic patients with incidentally discovered adrenal masses were included in this study (Fig. 1). The clinical characteristics of the patients are shown in Table 1.

Flow chart of follow-up for cancer patients with adrenal incidentaloma (AI). PET-CT, positron emission tomography-computed tomography; MRI, magnetic resonance imaging; FNA, fine needle aspiration.

Clinical Characteristics of Cancer Patients with AI (n=131)
Hormonal evaluation
Twelve or 9.2% of the patients had functioning masses. There were four pheochromocytomas, six cases of primary hyperaldosteronism, and two with subclinical Cushing syndrome. Out of 119 patients (90.8%) with nonfunctioning tumors, 33 underwent adrenalectomy and three had ultrasound-guided biopsy.
Pathologic evaluation
The reason for pathologic diagnosis were tumor size >4 cm (n=6), possible malignancy (n=11), and concurrent operation for primary cancer (n=19, lung lobectomy in one subject, hepatectomy in one, gastrectomy in four, colorectomy in two, and nephrectomy in 11).
Of the above 36 patients, 13 (38.2%) had pathologically proven adrenal metastasis. One patient with diffuse large B-cell lymphoma had bilateral adrenal masses, and histological examination was conducted through ultrasound guided biopsy. A total of six metastases (46.2%) were synchronous with primary cancer.
The primary site of cancers of pathologically proven metastasis were lung cancer (n=3), renal cell carcinoma (n=2), lymphoma (n=2), hepatocellular carcinoma (n=2), breast cancer (n=1), gastric cancer (n=1), rectal cancer (n=1), and neuroblastoma (n=1).
Differentiation between benign and metastatic adrenal masses
Fig. 2 shows a scattergram of the HU and size comparison between clinically suspicious metastasis and benign adenoma. When comparing patients with 13 metastatic lesions and those with 23 benign ones, the median ages of the two groups were comparable (56.0 vs. 60.0, P=0.649). Benign masses ranged in diameter from 8.0 to 45.0 mm (median, 20.0), and the mass size was also significantly different (P=0.02) from those of metastases, which varied from 15.0 to 68.0 mm (median size, 29.0) (Fig. 2A). The HU for benign adrenal masses ranged from –15 to 25 HU (median, 13) and were significantly lower (P<0.001) than those of malignant masses (median, 32 HU; range, 21 to 40) (Fig. 2B). Among 56 subjects who had adrenal mass with HU over 10, 21 (37.5%) performed adrenal CT to differentiate lipid-poor adrenal adenoma from non-adenomatous lesion. There were 15 clinically suspicious benign and six malignant lesions. All 15 clinically suspicious benign lesions demonstrated rapid washout defined as APW of >60% and RPW >40% (Fig. 3). Of the 131 subjects, 119 with nonfunctioning masses were followed up for a period of 3 to 131 months. During the follow-up period, none of the subjects developed functional tumors.

(A) Adrenal size and (B) Hounsfield unit (HU) for clinically suspicious benign (b) and metastasis (m).
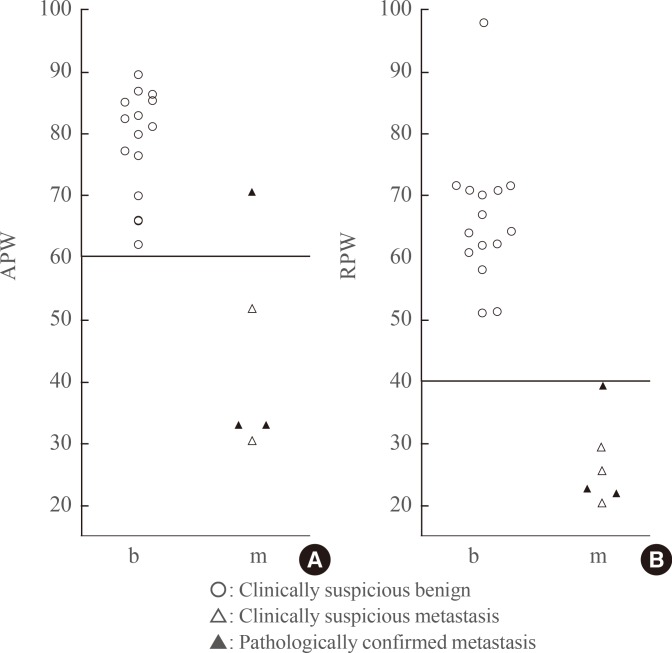
(A) Absolute percentage washout (APW) and (B) relative percentage washout (RPW) in case adrenal mass with Hounsfield unit over 10. b, clinically suspicious benign; m, clinically suspicious metastasis.
The optimal cut-off value of the tumor size for clinically suspicious metastasis was 22.0 mm (sensitivity 73.1%, specificity 78.5%) and the cut-off value of HU was 20.0 (sensitivity 95.0%, specificity 83.3%) under the ROC curve analysis (Fig. 4). The AUC value for the size and HU were 0.839 (95% confidence interval [CI], 0.761 to 0.900; P<0.001) and 0.955 (95% CI, 0.894 to 0.987; P<0.001), respectively. Increasing the size to 40 mm was associated with higher specificity (98.9%) but lower sensitivity (26.9%). Decreasing the threshold to 10 HU yielded a higher sensitivity (100%) but lower specificity (56.4%).
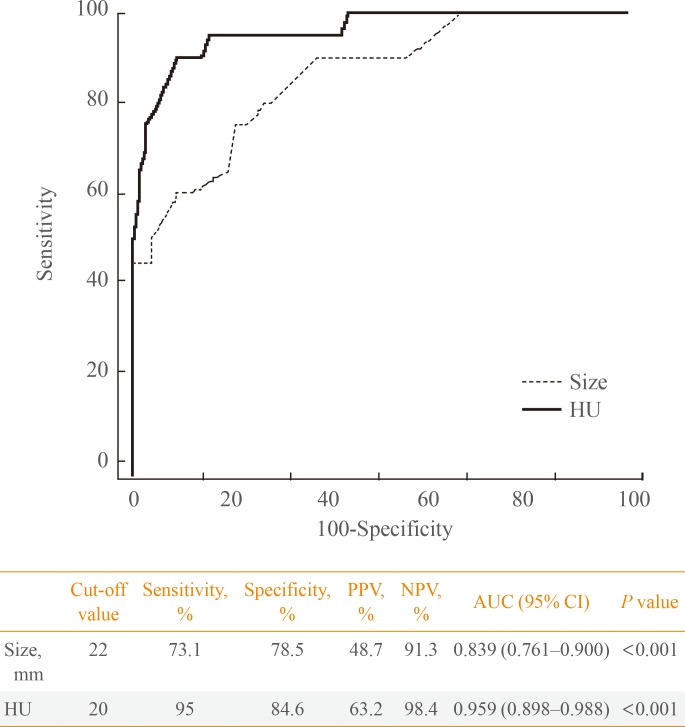
Receiver operating characteristic curve for adrenal mass defined as clinically suspicious metastasis. HU, Hounsfield unit; PPV, positive predictive value; NPV, negative predictive value; AUC, area under the curve; CI, confidence interval.
We confirmed that the AUC for HU (0.959) of the clinically suspicious metastasis was significantly higher than that for the size (0.839) using pairwise comparison of ROC curves (95% CI, 0.005 to 0.196; P=0.038). Moreover, the combination of size and HU showed the largest AUC (AUC, 0.971; 95% CI, 0.932 to 1.000; P<0.001). The AUC was significantly increased in the combination group (0.971) compared with size (0.839) alone (95% CI, 0.022 to 0.204; P=0.015); however, the difference of AUC between combination groups (0.971) and HU (0.939) was not significant (95% CI, –0.0003 to 0.0253; P=0.06).
DISCUSSION
This results of the retrospective study suggested that the pre-contrast HU and size of the adrenal mass on CT were useful to differentiate benign and metastatic lesions in 131 patients with extra-adrenal cancer. The ROC curve analysis showed the cut-off points for pre-contrast HU and size of the adrenal mass were 20 and 22 mm, respectively.
Previous studies have shown that a threshold value of <10 HU on the pre-contrast CT scans was employed to differentiate benign lesions from indeterminate lesions [91011]. Lipid-rich adenomas demonstrated low attenuation <10 HU due to the presence of intracellular lipids. Non-adenomatous lesions have higher attenuation values since they have a relatively lipid-poor cytoplasm. Non-calcified, non-hemorrhagic adrenal masses with attenuation values >43 HU were proposed to be malignant [12]. Considering these results were from on non-cancer patients, the cut-off value of 20 HU calculated in this study is a relevant threshold value for cancer patients.
In the present study, diameter greater than 22 mm was associated with metastatic adrenal lesions in cancer patients. Lesions larger than 4 cm in diameter are suggested as a surrogate for primary adrenal malignancy [13]; however, the size of metastatic lesions varies and can be bilateral. In fact, only four out of 13 patients with pathologically confirmed tumors showed lesions >4 cm in the present study. Even when metastatic adrenal lesions were clinically defined, the ROC curve analysis showed a cut-off value of 22 mm. These results suggest that the size of adrenal mass >2 cm detected in patients with an extra-adrenal cancer may be suspected for metastasis. However, the use of the size threshold alone has poor specificity regarding the high threshold (size <1.5 cm, specificity 45.2%, sensitivity, 88.5%) and poor sensitivity regarding the specificity (size >4 cm, specificity 98.9%, sensitivity 26.9%). The ROC curve for HU is located to the left of the tumor size, thereby suggesting a larger AUC and a better discriminatory ability. Therefore, HU was considered a better indicator to differentiate between metastasis and adenoma than the mass size, in accordance with previous studies [1114]. Furthermore, combination of HU and size might be more useful than size alone for screening of AI in oncologic patients. In this study, the lung was the most common primary malignant site, followed by the kidney, liver, and lymph node. These results are in close agreement with those of previous reports, including a study of 464 patients with adrenal metastases over a 30-year period [1516]. These indicate that the patient population in this study was not so distinct from other studies. However, this study has limitations, such as lack of contrast washout data in some cases and retrospective design of patients in a single center.
In conclusion, according to us, a pre-contrast value >20 HU on CT may be more useful than the mass size to differentiate metastasis from benign lesions detected incidentally in patients with extra-adrenal cancer.
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
