
Articles
- Page Path
- HOME > Endocrinol Metab > Volume 38(2); 2023 > Article
-
Original ArticleAdrenal gland Mortality and Severity of Coronavirus Disease 2019 in Patients with Long-Term Glucocorticoid Therapy: A Korean Nationwide Cohort Study
 Keypoint
Keypoint
The severity of COVID-19 in patients on long-term glucocorticoid treatment remains uncertain. This nationwide cohort study made a novel contribution by showing that the overall mortality rates were higher in this group than in the control group, even after adjusting for other factors. This increased risk was particularly notable in patients with underlying comorbidities. It is crucial to implement proactive measures to address the challenges posed by COVID-19, especially for individuals receiving long-term glucocorticoid treatment and those with multiple comorbidities. -
Eu Jeong Ku1
 , Keeho Song2, Kyoung Min Kim3, Gi Hyeon Seo4, Soon Jib Yoo5
, Keeho Song2, Kyoung Min Kim3, Gi Hyeon Seo4, Soon Jib Yoo5 -
Endocrinology and Metabolism 2023;38(2):253-259.
DOI: https://doi.org/10.3803/EnM.2022.1607
Published online: March 21, 2023
1Division of Endocrinology and Metabolism, Department of Internal Medicine, Chungbuk National University Hospital, Chungbuk National University College of Medicine, Cheongju, Korea
2Division of Endocrinology and Metabolism, Department of Internal Medicine, Konkuk University School of Medicine, Seoul, Korea
3Division of Endocrinology, Department of Internal Medicine, Yongin Severance Hospital, Yonsei University College of Medicine, Yongin, Korea
4Health Insurance Review and Assessment Service, Wonju, Korea
5Division of Endocrinology and Metabolism, Department of Internal Medicine, Bucheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- Corresponding authors: Soon Jib Yoo. Division of Endocrinology and Metabolism, Department of Internal Medicine, Bucheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 327 Sosa-ro, Wonmi-gu, Bucheon 14647, Korea Tel: +82-32-340-7011, Fax: +82-32-340-2039, E-mail: sjyoomt@gmail.com
- Gi Hyeon Seo. Health Insurance Review and Assessment Service, 60 Hyeoksin-ro, Wonju 26465, Korea Tel: +82-2-2182-2307, Fax: +82-33-811-7447, E-mail: seogih@gmail.com
Copyright © 2023 Korean Endocrine Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- The severity of coronavirus disease 2019 (COVID-19) among patients with long-term glucocorticoid treatment (LTGT) has not been established. We aimed to evaluate the association between LTGT and COVID-19 prognosis.
-
Methods
- A Korean nationwide cohort database of COVID-19 patients between January 2019 and September 2021 was used. LTGT was defined as exposure to at least 150 mg of prednisolone (≥5 mg/day and ≥30 days) or equivalent glucocorticoids 180 days before COVID-19 infection. The outcome measurements were mortality, hospitalization, intensive care unit (ICU) admission, length of stay, and mechanical ventilation.
-
Results
- Among confirmed patients with COVID-19, the LTGT group (n=12,794) was older and had a higher proportion of comorbidities than the control (n=359,013). The LTGT group showed higher in-hospital, 30-day, and 90-day mortality rates than the control (14.0% vs. 2.3%, 5.9% vs. 1.1%, and 9.9% vs. 1.8%, respectively; all P<0.001). Except for the hospitalization rate, the length of stay, ICU admission, and mechanical ventilation proportions were significantly higher in the LTGT group than in the control (all P<0.001). Overall mortality was higher in the LTGT group than in the control group, and the significance remained in the fully adjusted model (odds ratio [OR], 5.75; 95% confidence interval [CI], 5.31 to 6.23) (adjusted OR, 1.82; 95% CI, 1.67 to 2.00). The LTGT group showed a higher mortality rate than the control within the same comorbidity score category.
-
Conclusion
- Long-term exposure to glucocorticoids increased the mortality and severity of COVID-19. Prevention and early proactive measures are inevitable in the high-risk LTGT group with many comorbidities.
- Since the first case of new coronavirus called severe acute respiratory syndrome coronavirus 2, also known as coronavirus disease 2019 (COVID-19), occurred in December 2019, there have been 605 million cumulative cases worldwide and 6.49 million deaths [1,2]. Although the number of infected people is gradually decreasing because of the availability of COVID-19 vaccines and the application of the treatment, it is still too early to overlook the fact that the number of confirmed cases exceeds 450,000 per day worldwide, negatively affecting the health of the global population [1].
- As the risk of severe COVID-19 and adverse outcomes continues to increase, special care is needed, particularly for the elderly population and those at high-risk with underlying medical conditions, including diabetes mellitus, chronic kidney disease (CKD), cardiovascular disease (CVD), and other various chronic diseases [3-5]. Several guidelines for these populations have been released [6-9].
- In various chronic diseases such as rheumatoid arthritis (RA), chronic obstructive pulmonary disease (COPD), and asthma, long-term use of glucocorticoids inevitably leads to adrenal insufficiency [10,11]. Patients with adrenal insufficiency are considered at an increased risk of infection due to an altered immune system and an increased risk of infection-induced adrenal crisis, which can lead to death and serious complications [12]. As reported in a small case-control study, patients with adrenal insufficiency who were well-trained with an appropriate replacement strategy following “sick day rules” had similar rates and severity of COVID-19 infection as controls with intact adrenal function [13]. Nevertheless, considering the various adverse effects caused by the prolonged use of glucocorticoids and the underlying diseases of patients who need to continue long-term or/and high-dose regimens, concerns persist that people receiving long-term glucocorticoid treatment (LTGT) are vulnerable to infectious diseases. Moreover, the association between LTGT with a high-risk of adrenal insufficiency and the risk of mortality and severe outcomes among patients with COVID-19 remains unclear. Therefore, this study aimed to determine the mortality and other severe outcomes of COVID-19 in patients with LTGT compared to a control group using a Korean nationwide population-based database.
INTRODUCTION
- Ethical considerations
- This study was approved by the Institutional Review Board Committee of the Korean Health Insurance Review and Assessment Service as an exemption study (HIRA IRB 2022-054). The need for informed consent was waived as all data used in the National Health Insurance Service (NHIS) database were anonymized and de-identified before being provided.
- Data sources and study population
- In this retrospective cohort study, all patients with COVID-19 infection from January 2020 to September 2021 in the Korea NHIS database were included to evaluate outcomes of COVID-19 in patients with LTGT. In brief, the NHIS has secured nationwide COVID-19 cohort data by providing public health insurance to the entire population of South Korea. Heretofore, the government has provided free medical care by assigning a special code—“3/02” in MT043—to the type of National Disaster Medical Expense Subsidy when a patient is diagnosed with COVID-19 to prevent the spread of it via thorough infection control. Therefore, under the International Classification of Diseases, Tenth Revision (ICD-10), the following ICD-10 codes and specially assigned claim codes simultaneously were used to identify patients with COVID-19: B34.2 (coronavirus infection, unspecified site), U18.1 (novel coronavirus infection), U07.1 (COVID-19, virus identified), and U07.2 (COVID-19, virus not identified).
- Underlying diseases, including diabetes mellitus, hypertension, CVD, cerebral infarction or transient ischemic accident, CKD, COPD, asthma, and RA, were defined as at least one claim of either outpatient, inpatient, or both using each appropriate ICD-10 code within 1 year prior to the date of COVID-19 diagnosis.
- Operational definitions of the LTGT group and control group
- Given the National Institute for Health and Care Excellence guideline for patients at risk of systemic side effects from oral corticosteroids, LTGT was defined as a prescription of oral prednisolone ≥5 mg/day or the equivalent for at least 30 days from the previous 180 days to the time of diagnosis of COVID-19 [14]. The control group consisted of patients who had not been prescribed glucocorticoids for 180 days before the date of confirmed COVID-19 infection.
- Outcome measurements
- The primary outcome of this study was overall mortality among patients with LTGT compared with the control group after a diagnosis of COVID-19. The secondary endpoints included the following other severe COVID-19 results that were compared between the LTGT group and control group: hospitalization rates, need for admission to the intensive care unit (ICU), length of stay, and need for oxygen therapy, including mechanical ventilation.
- Statistical analysis
- Baseline characteristics and clinical outcomes of the study population are expressed as a number with percentage (%) and mean with standard deviation (SD). Continuous variables were compared between the two groups using the t test, whereas categorical variables were analyzed using the chi-square test or Fisher exact test as appropriate. The odds ratio (OR) with 95% confidence interval (CI) of mortality in patients with LTGT was calculated using logistic regression analysis. To further strengthen the mortality risk in the LTGT group, a multivariable-adjusted OR was generated in logistic regression analysis to compare the mortality rate between the groups after data were adjusted for age, sex, Charlson comorbidity index (CCI), and the following comorbidities: diabetes mellitus, hypertension, CVD, cerebrovascular disease, CKD, COPD, asthma, and RA. Kaplan-Meier survival curves were compared between the groups using the log-rank test, and subgroups were analyzed according to the CCI index (0, 1, and ≥2) of both groups to adjust the multiple comorbidities related to survival. The CCI score was calculated based on ICD-10 codes [15].
- Statistical significance was set at a two-sided P<0.05. All statistical analyses were performed using R version 4.1.1 (The R Project for Statistical Computing, Vienna, Austria).
METHODS
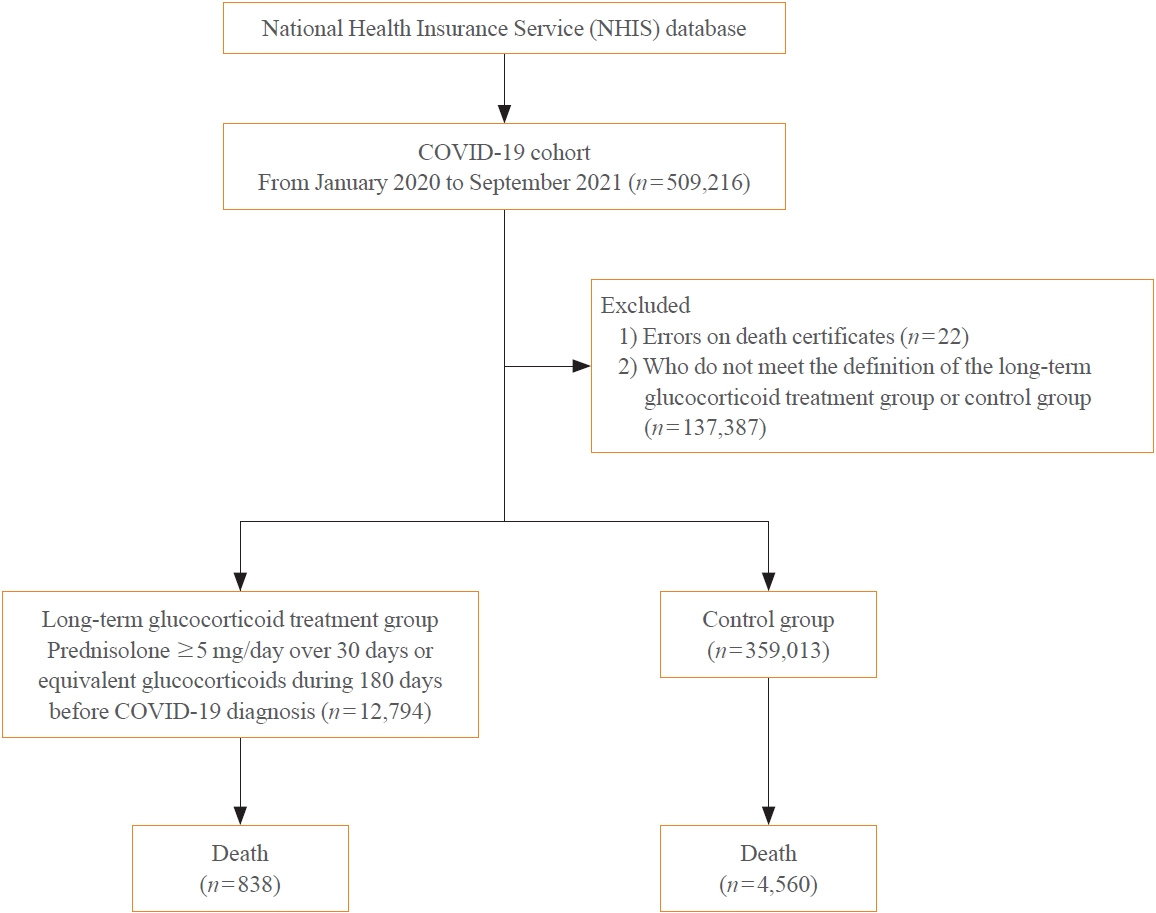
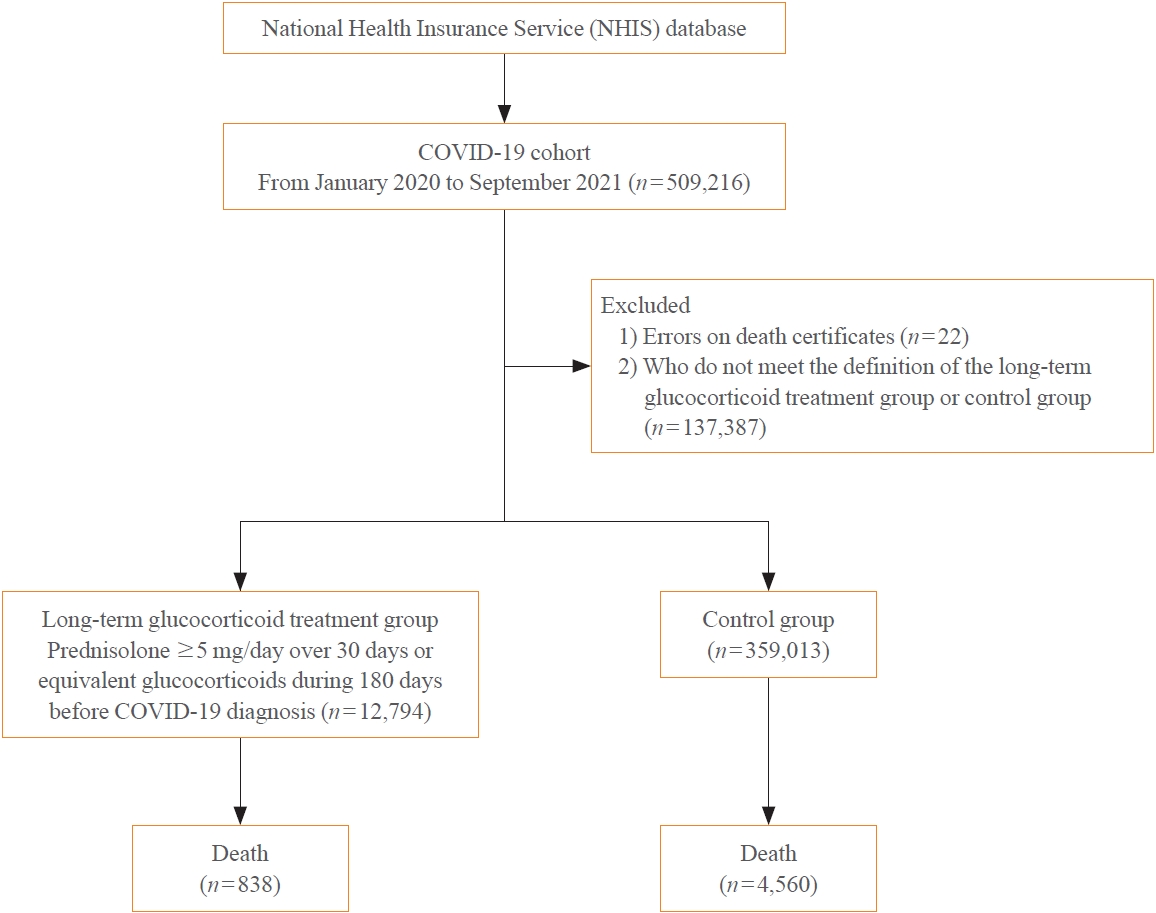
- Among the total 509,216 patients diagnosed with COVID-19 from January 2019 to September 2021, there were 12,794 and 359,013 patients in LTGT group and control group, respectively, after excluding those with a lack of baseline information (n=22) and patients who did not meet the inclusion criteria (n=137,387) (Fig. 1). The baseline characteristic of the study population at the time of diagnosis of COVID-19 are summarized in Table 1. The LTGT group was older than the control group (mean±SD age, 57.8±21.3 years vs. 40.7±21.3 years, P<0.001), and the proportion of men was slightly lower in the LTGT group than in the control group (50.3% vs. 52.5%, P<0.001). There were also significant differences in comorbidities between the groups. The LTGT group had a higher rate of accompanying diabetes mellitus, hypertension, CVD, and CKD than the control group. Additionally, the incidences of chronic inflammatory diseases such as COPD, asthma, and RA, each disease that requires glucocorticoids as treatment, were more than five times higher in the LTGT than in the control group (COPD, asthma, and RA: 10.4% vs. 1.1%, 21.7% vs. 4.8%, and 15.7% vs. 1.2%, respectively; all P<0.001).
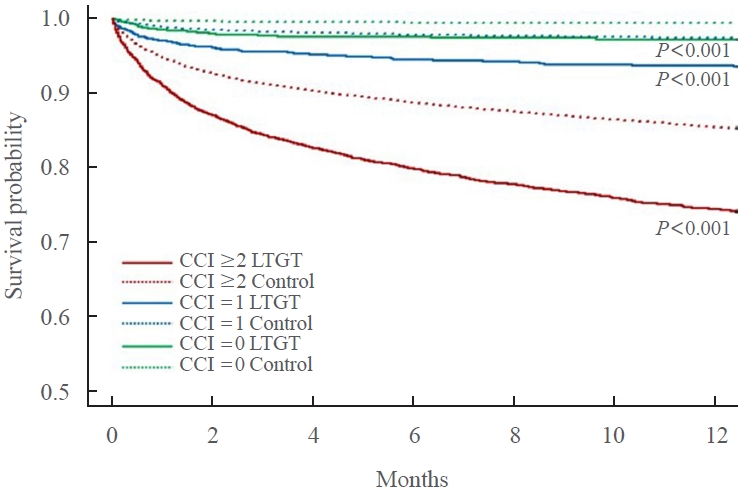
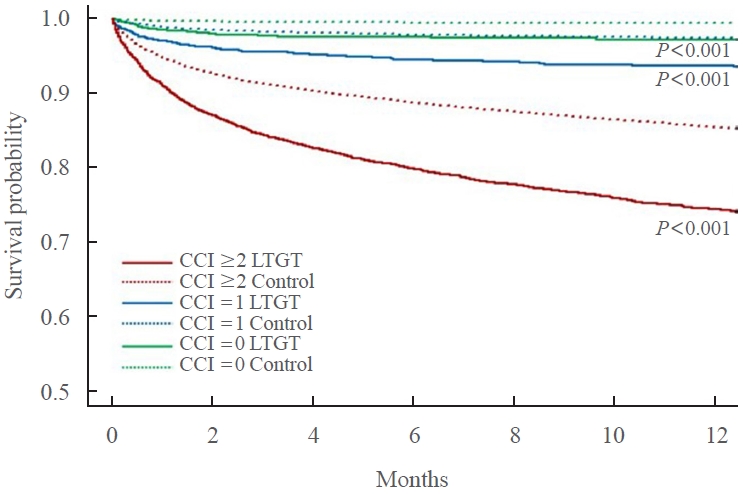
- Table 2 shows the treatment outcomes for COVID-19, including mortality. The hospitalization rate for COVID-19 was lower in the LTGT group than in the control group, but the ICU admission rate was more than doubled in the LTGT group than in the control group. The application of mechanical ventilation and simple oxygen therapy was also significantly higher in the LTGT group than in the control group. The length of hospitalization in the LTGT group was 19.2±26.7 days overall, which was longer than the 13.6±26.7 days in the control group, and the length of stay in the ICU was significantly longer in the LTGT group than in the control group (22.8±32.1 days vs. 19.0±32.1 days, P=0.017). In-hospital mortality was approximately 6.1 times higher in the LTGT group than in the control group (14.0% vs. 2.3%, P<0.001), and 30- and 90-day mortalities were 5.4 and 5.5 times higher in the LTGT group than in the control group, respectively (both P<0.001). The mortality rate, according to the CCI score, was significantly higher in the LTGT group than in the control group in all categories. Especially in the group with a CCI score ≥2, the LTGT group had a mortality rate of 6.1 times higher than the control group (P<0.001). Overall mortality in the LTGT group was higher (5.75; 95% CI, 5.31 to 6.23; P<0.001) than that in the control group, and the adjusted OR was significant at 1.82 (95% CI, 1.67 to 2.00; P<0.001) after adjusting for confounding factors including age, sex, the CCI score, and underlying comorbidities. The Kaplan-Meier curves for each CCI category in both groups are shown in Fig. 2. In the same CCI category, the LTGT group showed a significantly higher mortality than the control group (both P<0.001).
RESULTS
- This study evaluated the association between long-term glucocorticoid use and COVID-19 severity and mortality in patients diagnosed with COVID-19 in South Korea from January 2020 to September 2021. In this nationwide population-based study, the patients with LTGT showed significantly high mortality and severe COVID-19 outcomes. After adjusting for various confounding factors, the LTGT group showed a significantly higher proportion of comorbidities than the control group. Even taking this into account, it was important that the group treated with glucocorticoids for a long time had a 1.8-fold higher mortality rate than the control group. Especially in the high-risk group with a CCI score ≥2, the mortality gap between the LTGT group and control group widened by >6 times.
- Since the outbreak of the COVID-19 pandemic, several studies have shown an increased risk of adverse COVID-19 outcomes in patients with Cushing syndrome, a condition of elevated endogenous cortisol, and in patients receiving high-dose glucocorticoid therapy for chronic diseases, such as asthma and inflammatory bowel disease [16-18]. Prolonged exposure to iatrogenic glucocorticoids suppresses the hypothalamus-pituitary-adrenal axis, leading to secondary adrenal insufficiency [10,11]. The pivotal role of glucocorticoids in the deterioration of the immune system increase susceptibility to infection [19,20]. Additionally, patients with adrenal insufficiency are more likely to have an infection-induced adrenal crisis than those without, which is a serious complication that may lead to death [21,22]. In Italy, a tertiary center study of 279 patients with primary or secondary adrenal insufficiency who were properly trained with regular follow-up found that COVID-19 infection and severity had a similar pattern in those patients compared to controls [13]. However, as hypothesized, LTGT has been reported to be associated with a poor prognosis for COVID-19 [16-18,23]. According to a study of >80,000 patients with asthma in Israel, recent exposures to chronic systemic corticosteroids within approximately 4 months prior to COVID-19 infection were independent risk factors for severity and all-cause mortality [16]. Considering that the proportion of pre-existing chronic diseases, including COPD, asthma, and RA, were significantly higher in the LTGT group than in the control group in our study, recent previous long-term glucocorticoid exposure could lead to poor outcomes of COVID-19.
- To date, risk factors associated with COVID-19 mortality are older age, male sex, and underlying chronic diseases, e.g., hypertension, diabetes mellitus, COPD, renal disease, CVD, and malignancy [24-27]. We showed that patients who were exposed to at least 150 mg of prednisolone (≥5 mg/day and ≥30 days) or equivalent doses of glucocorticoids 180 days before the onset of COVID-19 had a mortality rate approximately 2-fold higher than the controls, even after controlling for various possible confounding factors. Our subgroup analysis by CCI category, a predictive indicator for mortality, highlighted adverse outcomes of COVID-19 with LTGT.
- Meanwhile, in our study, the hospitalization rate of LTGT was lower than that of the control group. At the beginning of the study period, the Korean government had a policy of hospitalizing and isolating all COVID-19-infected patients, regardless of the severity of their symptoms. Moreover, during the early period of the COVID-19 pandemic, many young and healthy people, including religious groups, were hospitalized after cluster infections in a local city [28]. These environmental factors surrounding COVID-19 may have contributed to the relatively higher hospitalization rate in the control group.
- There are some limitations to this study. First, since this study used claim data, information on laboratory results or vital signs was unavailable, so the operational definition of severe COVID-19 could only be determined by the application of oxygen therapy and invasive mechanical ventilation or admission to the ICU. Second, the cause of death provided by the National Statistical Office was not linked. However, mortality within 30 days after the diagnosis of COVID-19 is more likely to mean death due to COVID-19 rather than other diseases. Therefore, it is difficult to undermine the significance of our study results. Third, we were not able to identify the underlying diseases for LTGT. In particular, the results of this study did not include all chronic metabolic or inflammatory diseases. For example, dyslipidemia was not considered an independent variable. However, we tried to identify as many underlying conditions associated with the severity and mortality from COVID-19 in individuals as possible. The prevalence in Korea is estimated to be 300, 30, and 10 per 100,000 population for RA, systematic lupus erythematosus, and ankylosing spondylitis, respectively [29-31]. Therefore, in this study, RA was included as a representative autoimmune disease with a high possibility of LTGT. Even so, it is noteworthy that the mortality rate of the LTGT group was significantly higher than that of the control group, even after adjusting for age, sex, CCI score, and various comorbidities. Finally, the results should be carefully interpreted because not all long-term glucocorticoid users have adrenal insufficiency, and not all routes of administration of glucocorticoids other than oral, e.g., topical or inhaled, have been analyzed. Moreover, it is unknown whether the proper replacement measure by the sick day rule has been applied. Nevertheless, this study’s findings have important clinical implications in terms of raising awareness among clinicians and patients that various chronic diseases are prone to prolonged exposure to glucocorticoids, which can worsen the matter.
- In conclusion, this nationwide population-based case-control study showed that patients exposed to LTGT had severe COVID-19 outcomes, including increased mortality. Especially as the risk of LTGT increased greatly in the higher risk group with various underlying comorbidities, preemptive measures should be taken to overcome the COVID-19 pandemic.
DISCUSSION
-
Acknowledgements
- This study was supported by the Big Data Research from the Korean Endocrinology Society in 2022.
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conception or design: E.J.K. Acquisition, analysis, or interpretation of data: E.J.K., K.S., K.M.K., G.H.S., S.J.Y. Drafting the work or revising: E.J.K., G.H.S. Final approval of the manuscript: E.J.K., K.S., K.M.K., G.H.S., S.J.Y.
Article information
Values are expressed as mean±standard deviation or number (%). The Fisher exact test or t test was performed to compare data between the two groups. P<0.05 is considered significant.
LTGT, long-term glucocorticoid treatment; NHIS, National Health Insurance Service; COVID-19, coronavirus disease 2019; COPD, chronic obstructive pulmonary disease; CCI, Charlson comorbidity index.
Values are expressed as number (%) or mean±standard deviation. Mortality by the CCI score was 30-day mortality, expressed as a percentage of the number of deaths related to the number of patients in the CCI score category in each group. The Fisher exact test or t test was performed to compare data between the two groups. P<0.05 is considered significant.
COVID-19, coronavirus disease 2019; LTGT, long-term glucocorticoid treatment; CCI, Charlson comorbidity index; ICU, intensive care unit.
- 1. World Health Organization. WHO coronavirus (COVID-19) dashboard [Internet]. Geneva: WHO; 2022 [cited 2023 Feb 14]. Available from: https://covid19.who.int/.
- 2. He F, Deng Y, Li W. Coronavirus disease 2019: what we know? J Med Virol 2020;92:719–25.ArticlePubMedPMCPDF
- 3. Guan WJ, Liang WH, Zhao Y, Liang HR, Chen ZS, Li YM, et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: a nationwide analysis. Eur Respir J 2020;55:2000547.ArticlePubMedPMC
- 4. Hartmann-Boyce J, Rees K, Perring JC, Kerneis SA, Morris EM, Goyder C, et al. Risks of and from SARS-CoV-2 infection and COVID-19 in people with diabetes: a systematic review of reviews. Diabetes Care 2021;44:2790–811.ArticlePubMedPMCPDF
- 5. Jordan RE, Adab P, Cheng KK. COVID-19: risk factors for severe disease and death. BMJ 2020;368:m1198.ArticlePubMed
- 6. American Diabetes Association Professional Practice Committee. 4. Comprehensive medical evaluation and assessment of comorbidities: standards of medical care in diabetes-2022. Diabetes Care 2022;45(Suppl 1):S46–59.
- 7. Clerkin KJ, Fried JA, Raikhelkar J, Sayer G, Griffin JM, Masoumi A, et al. COVID-19 and cardiovascular disease. Circulation 2020;141:1648–55.ArticlePubMed
- 8. Ku CR, Jung KY, Ahn CH, Moon JS, Lee JH, Kim EH, et al. COVID-19 vaccination for endocrine patients: a position statement from the Korean Endocrine Society. Endocrinol Metab (Seoul) 2021;36:757–65.ArticlePubMedPMCPDF
- 9. Puig-Domingo M, Marazuela M, Yildiz BO, Giustina A. COVID-19 and endocrine and metabolic diseases. An updated statement from the European Society of Endocrinology. Endocrine 2021;72:301–16.ArticlePubMedPMCPDF
- 10. Borresen SW, Klose M, Baslund B, Rasmussen AK, Hilsted L, Friis-Hansen L, et al. Adrenal insufficiency is seen in more than one-third of patients during ongoing low-dose prednisolone treatment for rheumatoid arthritis. Eur J Endocrinol 2017;177:287–95.ArticlePubMed
- 11. Lipworth BJ. Adrenal insufficiency after treatment with fluticasone: second line controller treatment might have been tried. BMJ 2002;325:836.
- 12. Teblick A, Peeters B, Langouche L, Van den Berghe G. Adrenal function and dysfunction in critically ill patients. Nat Rev Endocrinol 2019;15:417–27.ArticlePubMedPDF
- 13. Carosi G, Morelli V, Del Sindaco G, Serban AL, Cremaschi A, Frigerio S, et al. Adrenal insufficiency at the time of COVID-19: a retrospective study in patients referring to a tertiary center. J Clin Endocrinol Metab 2021;106:e1354–61.ArticlePubMedPMCPDF
- 14. Mundell L, Lindemann R, Douglas J. Monitoring long-term oral corticosteroids. BMJ Open Qual 2017;6:e000209.ArticlePubMedPMC
- 15. Glasheen WP, Cordier T, Gumpina R, Haugh G, Davis J, Renda A. Charlson comorbidity index: ICD-9 update and ICD-10 translation. Am Health Drug Benefits 2019;12:188–97.PubMedPMC
- 16. Adir Y, Humbert M, Saliba W. COVID-19 risk and outcomes in adult asthmatic patients treated with biologics or systemic corticosteroids: nationwide real-world evidence. J Allergy Clin Immunol 2021;148:361–7.ArticlePubMedPMC
- 17. Brenner EJ, Ungaro RC, Gearry RB, Kaplan GG, Kissous-Hunt M, Lewis JD, et al. Corticosteroids, but not TNF antagonists, are associated with adverse COVID-19 outcomes in patients with inflammatory bowel diseases: results from an International Registry. Gastroenterology 2020;159:481–91.ArticlePubMedPMC
- 18. Serban AL, Ferrante E, Carosi G, Indirli R, Arosio M, Mantovani G. COVID-19 in Cushing disease: experience of a single tertiary centre in Lombardy. J Endocrinol Invest 2021;44:1335–6.ArticlePubMedPMCPDF
- 19. Bancos I, Hazeldine J, Chortis V, Hampson P, Taylor AE, Lord JM, et al. Primary adrenal insufficiency is associated with impaired natural killer cell function: a potential link to increased mortality. Eur J Endocrinol 2017;176:471–80.ArticlePubMedPMC
- 20. Isidori AM, Venneri MA, Graziadio C, Simeoli C, Fiore D, Hasenmajer V, et al. Effect of once-daily, modified-release hydrocortisone versus standard glucocorticoid therapy on metabolism and innate immunity in patients with adrenal insufficiency (DREAM): a single-blind, randomised controlled trial. Lancet Diabetes Endocrinol 2018;6:173–85.ArticlePubMed
- 21. Arlt W, Baldeweg SE, Pearce SH, Simpson HL. Endocrinology in the time of COVID-19: management of adrenal insufficiency. Eur J Endocrinol 2020;183:G25–32.ArticlePubMedPMCPDF
- 22. Stewart PM, Biller BM, Marelli C, Gunnarsson C, Ryan MP, Johannsson G. Exploring inpatient hospitalizations and morbidity in patients with adrenal insufficiency. J Clin Endocrinol Metab 2016;101:4843–50.ArticlePubMedPDF
- 23. Hisamatsu T. Management of inflammatory bowel disease during the COVID-19 pandemic. Immunol Med 2022;45:128–35.ArticlePubMed
- 24. GBD 2019 Viewpoint Collaborators. Five insights from the Global Burden of Disease Study 2019. Lancet 2020;396:1135–59.PubMedPMC
- 25. Grasselli G, Greco M, Zanella A, Albano G, Antonelli M, Bellani G, et al. Risk factors associated with mortality among patients with COVID-19 in intensive care units in Lombardy, Italy. JAMA Intern Med 2020;180:1345–55.PubMed
- 26. Kim L, Garg S, O’Halloran A, Whitaker M, Pham H, Anderson EJ, et al. Risk factors for intensive care unit admission and in-hospital mortality among hospitalized adults identified through the US coronavirus disease 2019 (COVID-19)-associated hospitalization surveillance network (COVID-NET). Clin Infect Dis 2021;72:e206–14.ArticlePubMedPMCPDF
- 27. Parohan M, Yaghoubi S, Seraji A, Javanbakht MH, Sarraf P, Djalali M. Risk factors for mortality in patients with Coronavirus disease 2019 (COVID-19) infection: a systematic review and meta-analysis of observational studies. Aging Male 2020;23:1416–24.ArticlePubMed
- 28. Korea Disease Control and Prevention Agency. COVID-19 dashboard [Internet]. Sejong: Ministry of Health and Welfare; 2023 [cited 2023 Feb 14]. Available from: https://ncov.kdca.go.kr/.
- 29. Won S, Cho SK, Kim D, Han M, Lee J, Jang EJ, et al. Update on the prevalence and incidence of rheumatoid arthritis in Korea and an analysis of medical care and drug utilization. Rheumatol Int 2018;38:649–56.ArticlePubMedPDF
- 30. Bae EH, Lim SY, Han KD, Jung JH, Choi HS, Kim HY, et al. Trend of prevalence and incidence of systemic lupus erythematosus in South Korea, 2005 to 2015: a nationwide population-based study. Korean J Intern Med 2020;35:652–61.ArticlePubMedPMCPDF
- 31. Park JS, Hong JY, Park YS, Han K, Suh SW. Trends in the prevalence and incidence of ankylosing spondylitis in South Korea, 2010-2015 and estimated differences according to income status. Sci Rep 2018;8:7694.ArticlePubMedPMCPDF
References
Figure & Data
References
Citations
- Glucocorticoids as a Double-Edged Sword in the Treatment of COVID-19: Mortality and Severity of COVID-19 in Patients Receiving Long-Term Glucocorticoid Therapy
Eun-Hee Cho
Endocrinology and Metabolism.2023; 38(2): 223. CrossRef - Pituitary Diseases and COVID-19 Outcomes in South Korea: A Nationwide Cohort Study
Jeonghoon Ha, Kyoung Min Kim, Dong-Jun Lim, Keeho Song, Gi Hyeon Seo
Journal of Clinical Medicine.2023; 12(14): 4799. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-
- Related articles
-
- Increased Risk of Hip Fracture in Patients with Acromegaly: A Nationwide Cohort Study in Korea
- Glucocorticoids as a Double-Edged Sword in the Treatment of COVID-19: Mortality and Severity of COVID-19 in Patients Receiving Long-Term Glucocorticoid Therapy
- Risk and Risk Factors for Postpartum Type 2 Diabetes Mellitus in Women with Gestational Diabetes: A Korean Nationwide Cohort Study

