Articles
- Page Path
- HOME > Endocrinol Metab > Volume 38(1); 2023 > Article
-
Original ArticleThyroid Lower Thyroid Cancer Mortality in Patients Detected by Screening: A Meta-Analysis
 Keypoint
Keypoint
This meta-analysis compared incidental and non-incidental thyroid cancers to assess the impact of thyroid cancer screening on clinical outcomes. The findings indicate that patients with incidental thyroid cancer had less aggressive tumor characteristics and lower risks of recurrence and mortality rates. This study provides compelling evidence for the benefits of early detection of thyroid cancer compared to symptomatic diagnosis. These results suggest that thyroid cancer screening may be an effective tool in improving clinical outcomes for patients. -
Shinje Moon1*
 , Young Shin Song2*, Kyong Yeun Jung3, Eun Kyung Lee4, Young Joo Park5,6
, Young Shin Song2*, Kyong Yeun Jung3, Eun Kyung Lee4, Young Joo Park5,6 -
Endocrinology and Metabolism 2023;38(1):93-103.
DOI: https://doi.org/10.3803/EnM.2023.1667
Published online: February 27, 2023
1Department of Internal Medicine, Hallym University Kangnam Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea
2Department of Internal Medicine, CHA Bundang Medical Center, CHA University School of Medicine, Seongnam, Korea
3Department of Internal Medicine, Nowon Eulji Medical Center, Eulji University, Seoul, Korea
4Department of Internal Medicine, Center for Thyroid Cancer, National Cancer Center, Goyang, Korea
5Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea
6Department of Molecular Medicine and Biopharmaceutical Sciences Graduate School of Convergence Science and Technology, Seoul National University, Seoul, Korea
- Corresponding authors: Eun Kyung Lee Department of Internal Medicine, Center for Thyroid Cancer, National Cancer Center, 323 Ilsan-ro, Ilsandong-gu, Goyang 10408, Korea Tel: +82-31-920-1743, Fax: +82-31-920-2798, E-mail: eklee@ncc.re.kr
- Kyong Yeun Jung Department of Internal Medicine, Nowon Eulji Medical Center, Eulji University, 68 Hangeulbiseong-ro, Nowon-gu, Seoul 01830, Korea Tel: +82-2-970-8816, Fax: +82-2-970-8865, E-mail: yeun6486@gmail.com
- *These authors contributed equally to this work.
Copyright © 2023 Korean Endocrine Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- Thyroid cancer screening has contributed to the skyrocketing prevalence of thyroid cancer. However, the true benefit of thyroid cancer screening is not fully understood. This study aimed to evaluate the impact of screening on the clinical outcomes of thyroid cancer by comparing incidental thyroid cancer (ITC) with non-incidental thyroid cancer (NITC) through a meta-analysis.
-
Methods
- PubMed and Embase were searched from inception to September 2022. We estimated and compared the prevalence of high-risk features (aggressive histology of thyroid cancer, extrathyroidal extension, metastasis to regional lymph nodes or distant organs, and advanced tumor-node-metastasis [TNM] stage), thyroid cancer-specific death, and recurrence in the ITC and NITC groups. We also calculated pooled risks and 95% confidence intervals (CIs) of the outcomes derived from these two groups.
-
Results
- From 1,078 studies screened, 14 were included. In comparison to NITC, the ITC group had a lower incidence of aggressive histology (odds ratio [OR], 0.46; 95% CI, 0.31 to 0.7), smaller tumors (mean difference, −7.9 mm; 95% CI, −10.2 to −5.6), lymph node metastasis (OR, 0.64; 95% CI, 0.48 to 0.86), and distant metastasis (OR, 0.42; 95% CI, 0.23 to 0.77). The risks of recurrence and thyroid cancer-specific mortality were also lower in the ITC group (OR, 0.42; 95% CI, 0.25 to 0.71 and OR, 0.46; 95% CI, 0.28 to 0.74) than in the NITC group.
-
Conclusion
- Our findings provide important evidence of a survival benefit from the early detection of thyroid cancer compared to symptomatic thyroid cancer.
- The incidence of thyroid cancer has risen worldwide during the last three decades [1]. The observed increase in thyroid cancer may be attributable to the increase in incidentally detected subclinical microcarcinomas, rather than a real change in incidence [2,3]. The rapid increase in the incidence of thyroid cancer in the Korean population has been substantial, and a previous study argued that 90% of thyroid cancer cases in South Korean women between 2008 and 2012 were attributable to overdiagnosis, despite the non-inclusion of thyroid cancer screening in the national screening program [4]. In recent years, there has been intensified debate regarding the role of thyroid ultrasound screening in detecting thyroid cancer.
- The importance of a cancer screening program relies on its proven net benefit. According to the United States Preventive Services Task Force (USPSTF), the benefit is assessed in terms of five aspects: the screening effectiveness or accuracy, the benefits or harms of screening, and the benefits and harms of treatment [5]. To evaluate the benefits of thyroid cancer screening, associated experts reviewed references in the literature and assessed the evidence; however, few studies dealing with the benefits and harms of thyroid cancer screening were found [6]. Furthermore, the most important question—whether screening leads to a reduced risk of thyroid cancer-specific mortality— could not be answered yet [7].
- The necessity or uselessness of thyroid cancer screening has been investigated using outcomes derived from retrospective observational studies, but the extraordinarily good prognosis of thyroid cancer, the wide spectrum of definitions of thyroid incidentalomas, and the diverse sociomedical circumstances of the studied populations have yielded inconsistent results. This study aimed to evaluate the impact of screening on the outcomes of thyroid cancer through a comparison between the outcomes of incidental thyroid cancer (ITC) and non-incidental thyroid cancer (NITC). First, we estimated the prevalence of aggressive histologic features in ITC and NITC. Second, we compared the thyroid cancer-specific mortality and recurrence rates between ITC and NITC.
INTRODUCTION
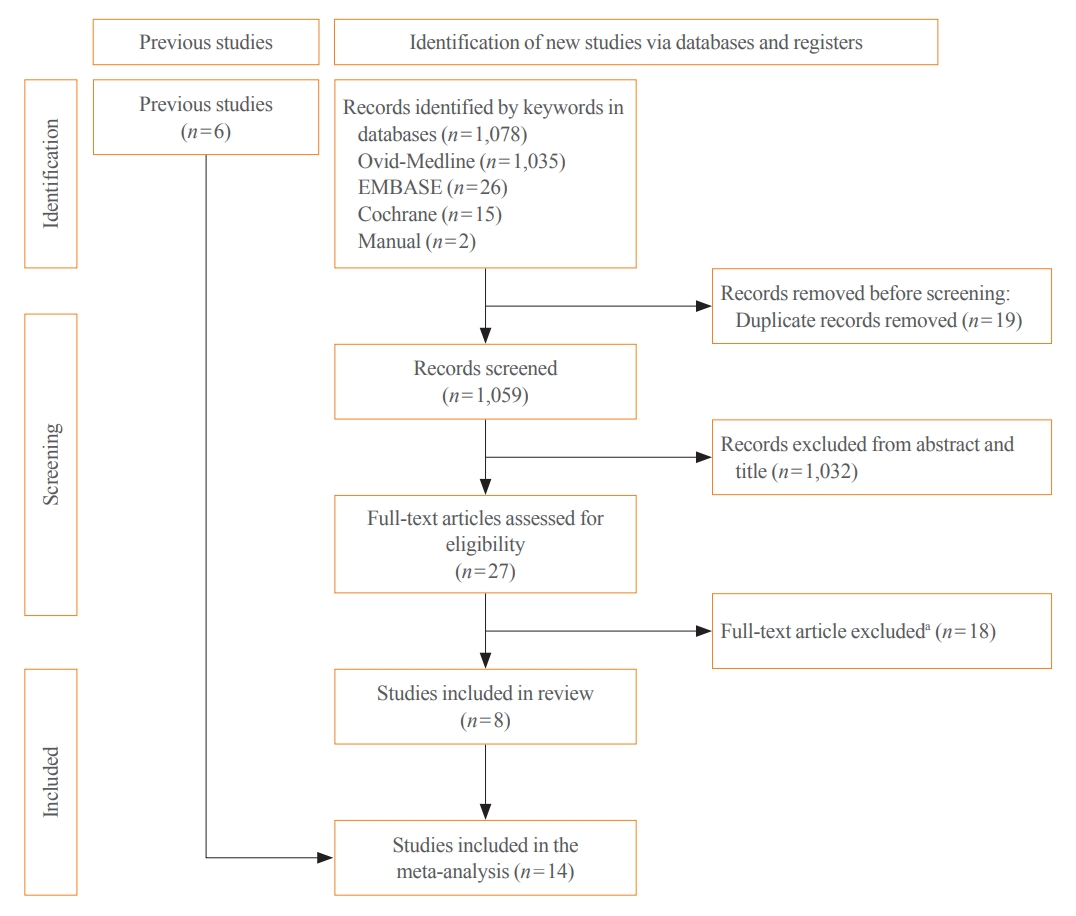
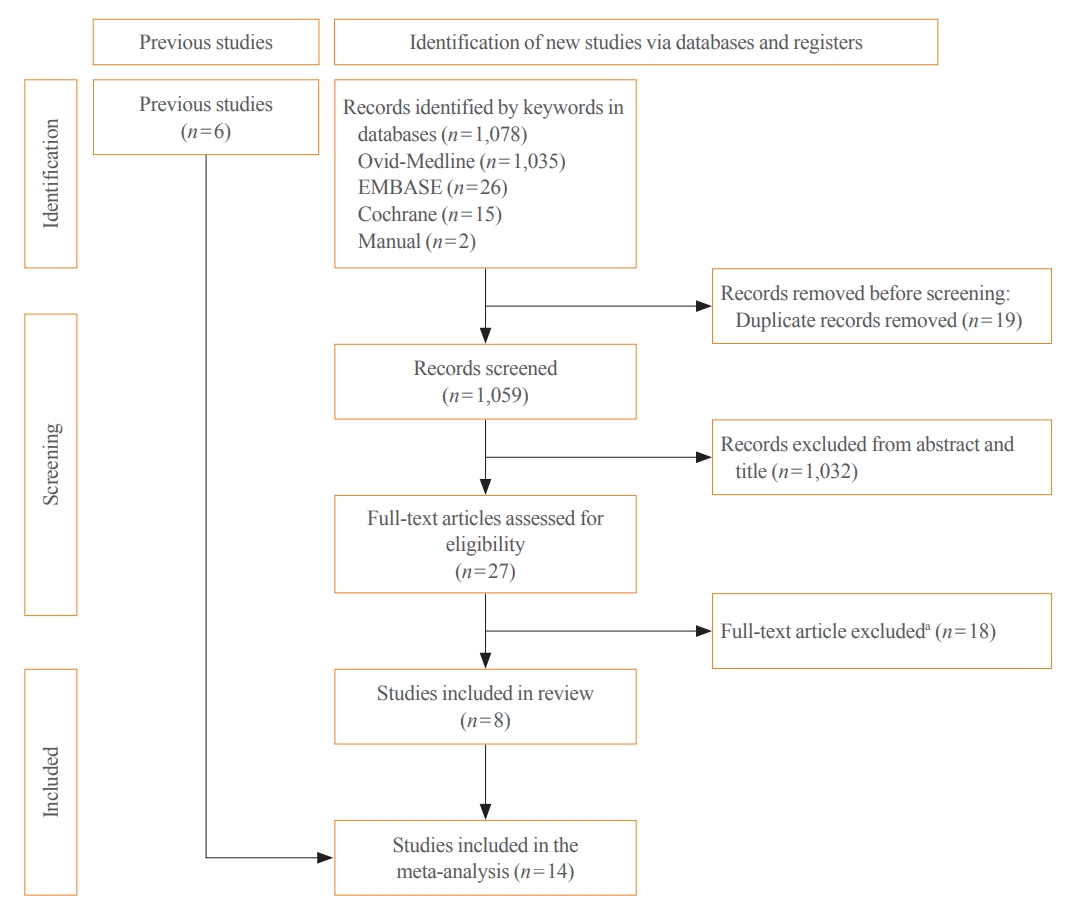
- For the purposes of this study, ITC was defined as an unexpected thyroid cancer incidentally detected by imaging methods (ultrasound, computed tomography [CT]/magnetic resonance imaging [MRI], and 18F-fludeoxyglucose [FDG] positron emission tomography [PET]/CT) or an analysis of a surgical pathology specimen. NITC was defined as thyroid cancer that had been detected due to clinical signs or symptoms (palpable thyroid lump, voice change or difficulty in swallowing, abnormality on a physical examination by a physician, and so on). This meta-analysis was performed following the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines (Supplemental Tables S1, S2) [8]. The flow diagram is shown in Fig. 1. The study protocol was registered in the Prospective Register of Systematic Reviews (number CRD42022365478).
- Search strategy and selection criteria
- We performed a systematic literature search through Ovid-MEDLINE, Embase, and the Cochrane Library for studies published since 2012. Studies prior to 2012 that were included in the 2012 National Evidence-based Healthcare Collaborating Agency (NECA) report [9] (n=3) and studies included in a recent systematic review [10] but not included in our search results (n=3) were manually added. The search started on August 29, 2022 and finished on September 7, 2022. Previous reviews were evaluated, and individual articles included therein were eligible for the present review. Search terms were created using the PICO structure as follows. The patients (P) were all individuals diagnosed with thyroid cancer. The intervention (I) was a thyroid imaging test with the intention of screening or another purpose. The comparator (C) was palpation of the thyroid gland or thyroid imaging test due to thyroid disease-related symptoms. The outcomes (O) comprised findings on clinicopathologic reports, including histology, tumor size, extrathyroidal extension (ETE), lymph node metastasis, distant metastasis, and tumornode-metastasis (TNM) stage, as well as the recurrence and thyroid cancer-specific mortality rates. The study design was a case-control design. The search terms and electronic search strategy are summarized in Supplemental Table S3.
- Duplicates were filtered through an automated function of the Endnote X9 citation manager and then manually searched. After removing duplicates, the titles and abstracts of the initial search results were screened, and non-English language publications were excluded. The full texts of the remaining articles were independently assessed by four investigators (S.M., Y.S.S., K.Y.J., and E.K.L.). Any discrepancies were resolved by discussion and consensus between the two researchers.
- Data extraction and management
- Data sets were extracted from each eligible study by four independent reviewers (S.M., Y.S.S., K.Y.J., and E.K.L.). The required information included author name, publication year, study design, country, the total number of patients and controls, the mean age of subjects, the sex ratio, histology, clinicopathologic characteristics, recurrence, and thyroid cancer-specific mortality for both groups. Discrepancies between the reviewers regarding study eligibility were resolved by discussion.
- Quality assessment and risk of bias
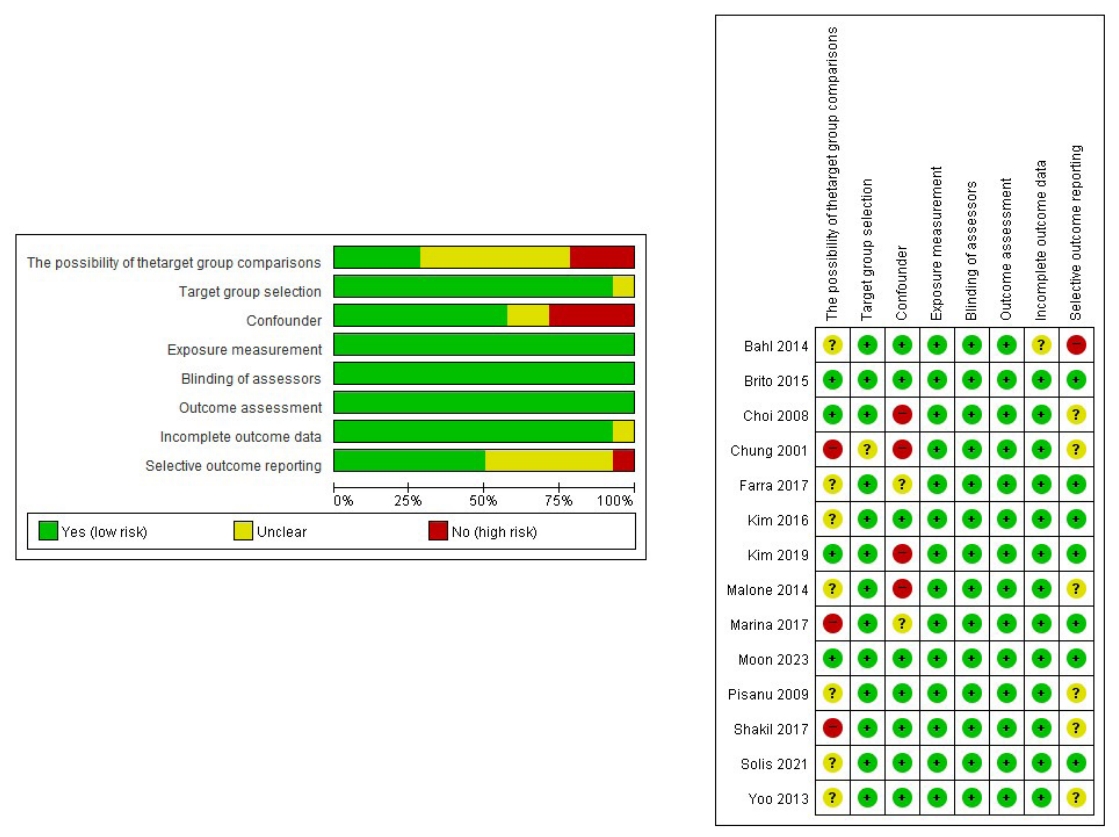
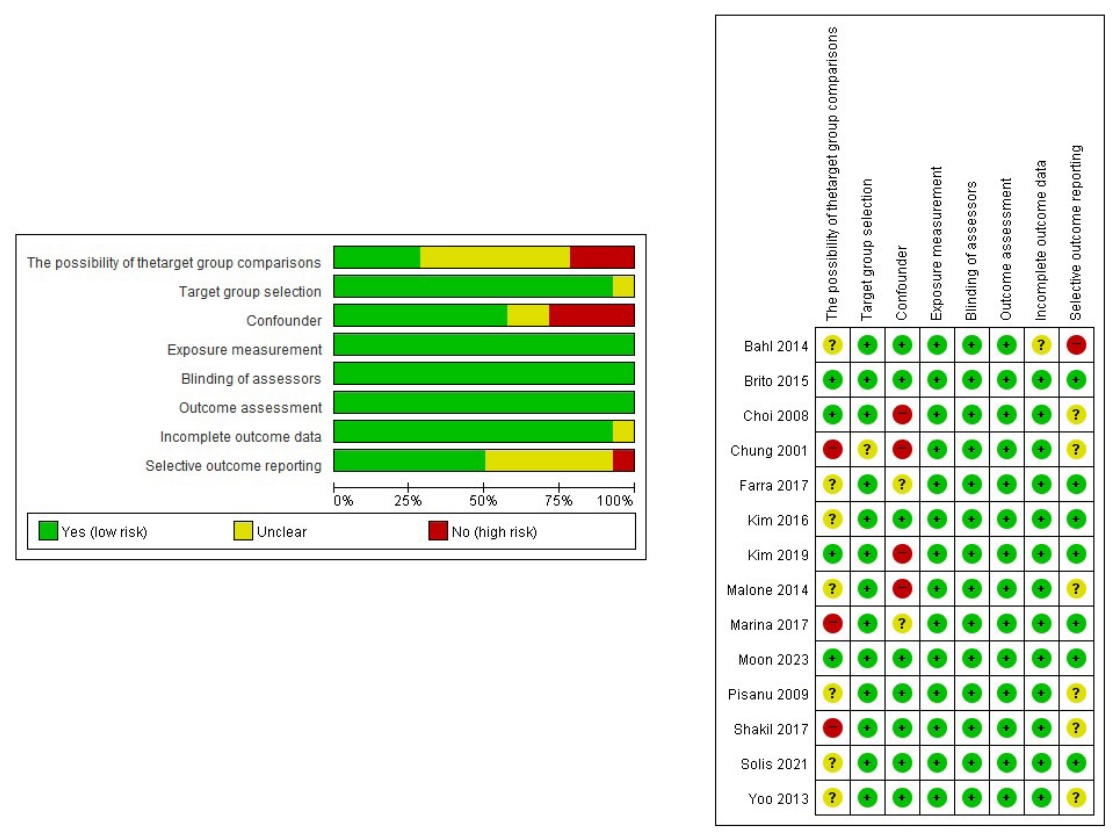
- The quality of the included studies and the risk of bias were assessed using the Cochrane risk of bias criteria (Risk of Bias Assessment of Non-randomized Studies [RoBANS] version 2.0), which included: (1) selection of participants, (2) confounding variables, (3) measurement of intervention, (4) blinding for outcome assessment, (5) incomplete outcome data, and (6) selective outcome reporting; these parameters were independently assessed by four reviewers (S.M., Y.S.S., K.Y.J., and E.K.L.). Any discrepancies were resolved by discussion. The quality of the 14 included studies was evaluated using RoBANS version 2.0 (Fig. 2).
- Statistical methods
- Comparisons of pathologic staging, recurrence rate, and thyroid cancer mortality were expressed as risk ratios and 95% confidence intervals (CIs). The heterogeneity of the studies was tested using the Higgins I2 statistic. I2 values of 25%, 50%, and 75% represented low, moderate, and high heterogeneity, respectively. If the I2 value was ≥50%, a random-effect model was used; if I2 was <50%, a fixed-effect model was used. Publication bias was investigated with the Egger test and by a visual evaluation of the funnel plot (Supplemental Fig. S1). A sensitivity analysis was conducted to determine the robustness of outcomes through repeated meta-analyses after excluding each study (Supplemental Fig. S2). Statistical analyses were performed with Comprehensive Meta-Analysis software version 3 (Biostat Inc., Englewood, NJ, USA) and R version 3.1.0 (R Foundation for Statistical Computing, Vienna, Austria; www.rproject.org). P values <0.05 were considered statistically significant.
METHODS
- Study characteristics
- The literature search yielded 1,078 studies. After the exclusion of 19 duplicate studies and 1,032 studies that did not meet the inclusion criteria, 14 studies [11-24] were finally included in the meta-analysis (Fig. 1). The characteristics of each study are summarized in Table 1. A total of 9,432 participants with thyroid cancer were enrolled, of whom 5,091 (53.9%) were incidentally diagnosed with thyroid cancer. Among them, 13 studies reported clinicopathologic results and six studies provided longitudinal data for recurrence or thyroid cancer-specific mortality in ITC and NITC. Five studies were conducted in Korea, six in America, and three in Europe.
- Risk of bias assessment
- The results of the risk of bias assessment using RoBANS are summarized in Fig. 2. (1) Regarding participant selection, four of the 14 case-control studies had a low risk in selection of participants, while three studies had a high-risk of bias due to an inadequate control group. The remaining seven studies were unclear. (2) Eight studies had a low-risk of bias due to confounders, while four had high-risk. Two studies were unclear. (3) All studies had a low-risk of bias due to measurement of intervention. (4) All studies showed a low-risk of bias due to blinding for outcome assessment or inadequate outcome assessment. (5) Thirteen studies had a low-risk of bias due to incomplete outcome data, and one was unclear. (6) For selective outcome reporting, seven studies were at a low-risk of bias, one at high-risk, and six at unclear risk.
- Comparison of pathologic characteristics between ITC and NITC
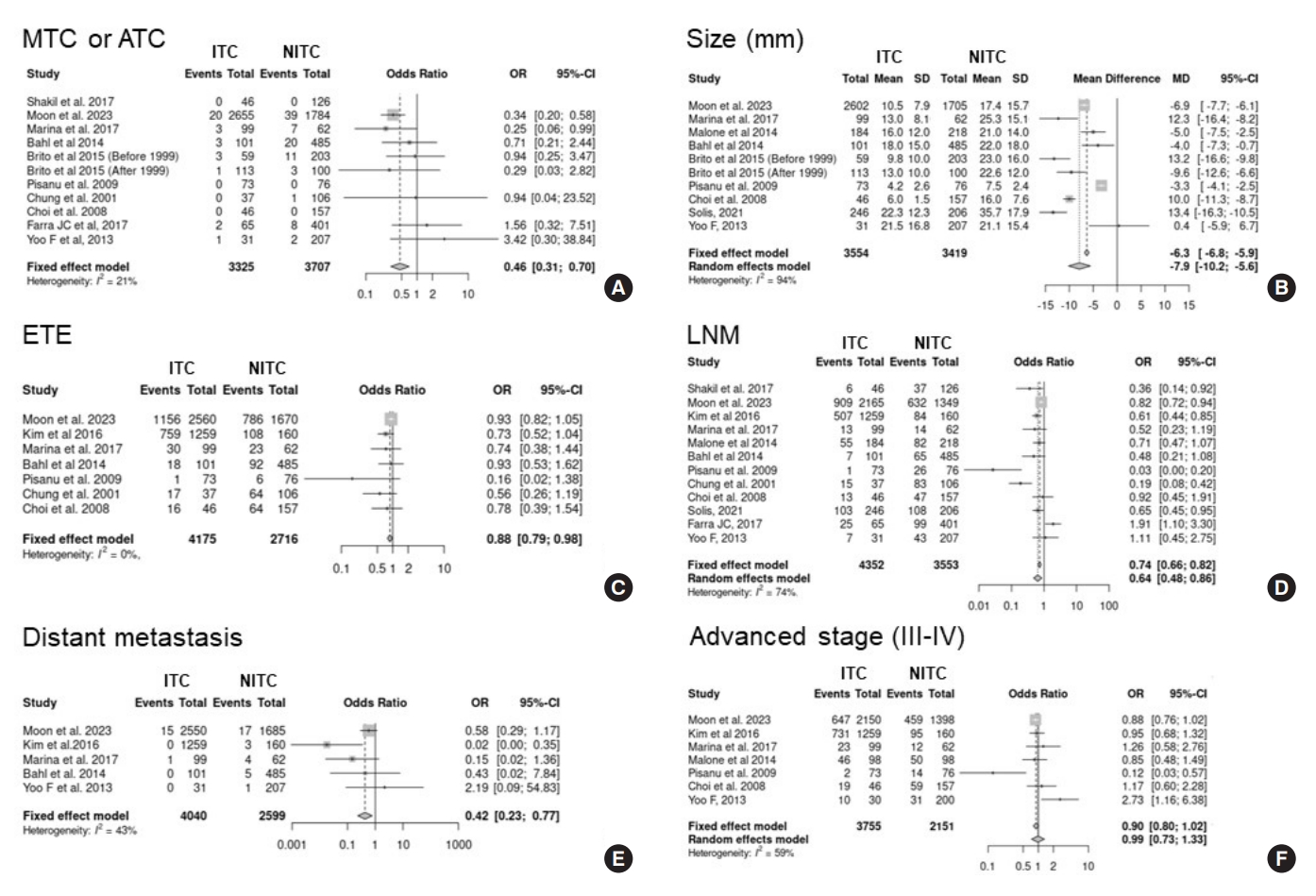
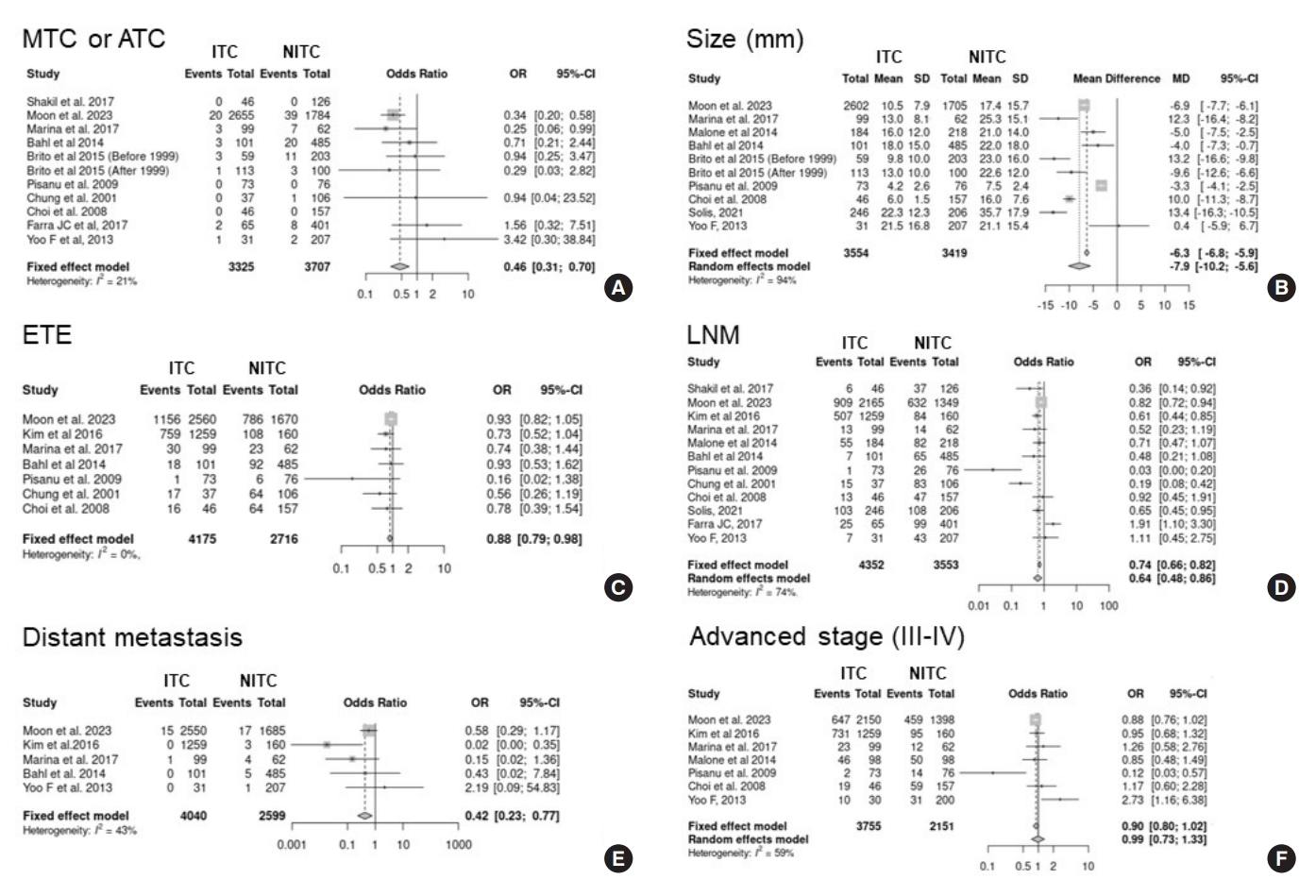
- To compare the distribution of aggressive histology between ITC and NITC, 10 studies were analyzed. The incidence of aggressive histology of thyroid cancer (medullary thyroid cancer or anaplastic thyroid cancer) was significantly lower in ITC than in NITC (odds ratio [OR], 0.46; 95% CI, 0.31 to 0.7) (Fig. 3A). Heterogeneity was not significant among these studies (I2=21%).
- Nine studies were included in the meta-analysis of tumor size in ITC and NITC. The mean difference between ITC and NITC was −7.9 mm (95% CI, −10.2 to −5.6), and I2 was 94%, indicating significant heterogeneity (Fig. 3B). The funnel plot was symmetrical, and publication bias was not detected (Egger test, P=0.315) (Supplemental Fig. S1). In the sensitivity analysis, the significance of the results did not change even after each study was removed, and no outliers were observed (Supplemental Fig. S2).
- To compare the proportion of ETE in ITC and NITC, seven studies were included. The ITC group had a lower risk of ETE (OR, 0.88; 95% CI, 0.79 to 0.98) (Fig. 3C). Heterogeneity was not significant among these studies (I2=0%); however, the funnel plot was asymmetrical and significant publication bias was detected (Egger test, P=0.019). The trim-and-fill method was conducted to adjust for publication bias and showed that statistical significance disappeared after adding three estimated missing studies (OR, 0.91; 95 % CI, 0.82 to 1.01) (Supplemental Fig. S1). The sensitivity analysis showed robust results from repeated analyses after excluding each study (Supplemental Fig. S2).
- Twelve studies were included in the meta-analysis of lymph node metastasis. The ITC group had a lower risk of lymph node metastasis (OR, 0.64; 95% CI, 0.48 to 0.86) compared to the NITC group, and I2 was 74%, indicating significant heterogeneity (Fig. 3D). The funnel plot was symmetrical, and publication bias was not significant (Egger test, P=0.134) (Supplemental Fig. S1). In the sensitivity analysis, the significance of the results did not change even after each study was removed, and no outliers were observed (Supplemental Fig. S2). In addition, lymph node metastasis was divided into central and lateral metastasis, and a meta-analysis was performed of the four studies that contained this information. The risk of central lymph node metastasis was not significantly different between the two groups (OR, 0.69; 95% CI, 0.38 to 1.24), but that of lateral lymph node metastasis was lower in the ITC group (OR, 0.31; 95% CI, 0.21 to 0.44) (Supplemental Fig. S3).
- Five studies were included in the meta-analysis of distant metastasis. The ITC group had a lower risk of distant metastasis (OR, 0.42; 95% CI, 0.23 to 0.77) than the NITC group, without significant heterogeneity (I2=43%) (Fig. 3E).
- Seven studies were included in the meta-analysis of TNM stage. The OR for advanced TNM stage (III to IV) was not significantly higher in the ITC group than in the NITC group, and there was significant heterogeneity (OR, 0.99; 95% CI, 0.73 to 1.33; I2=59%) (Fig. 3F).
- Mortality and recurrence rate in ITC and NITC
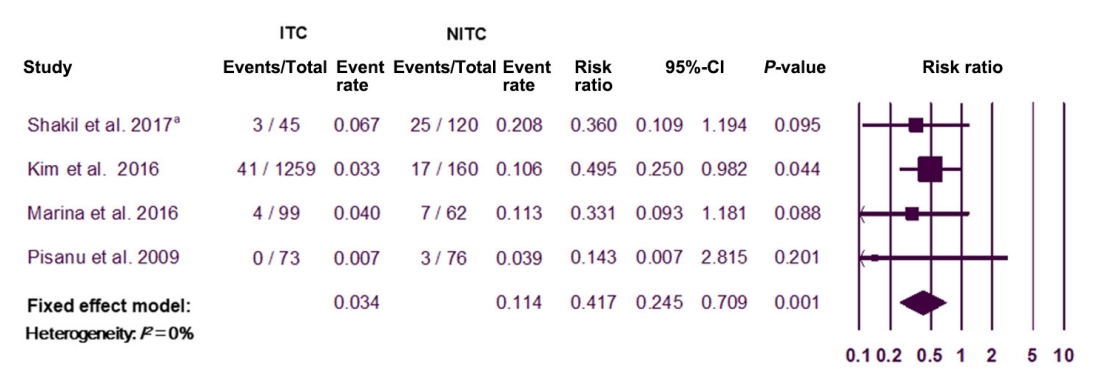
- Four studies were included in the meta-analysis of the recurrence rate in the ITC and NITC groups. The overall recurrence rate was 3.4% in the ITC group, versus 11.4% in the NITC group. In comparison with the NITC group, the ITC group had a significantly lower risk of recurrence (OR, 0.42; 95% CI, 0.25 to 0.71) (Fig. 4). Although no significant heterogeneity was found among these studies (I2=0%), the funnel plot was asymmetrical, and significant publication bias was detected (Egger’s test, P=0.01). The trim-and-fill method was conducted to adjust for publication bias and showed that statistical significance remained after adding two estimated missing studies (OR, 0.46; 95% CI, 0.28 to 0.74) (Supplemental Fig. S1). The sensitivity analysis showed robust results from repeated analyses after excluding each study (Supplemental Fig. S2).
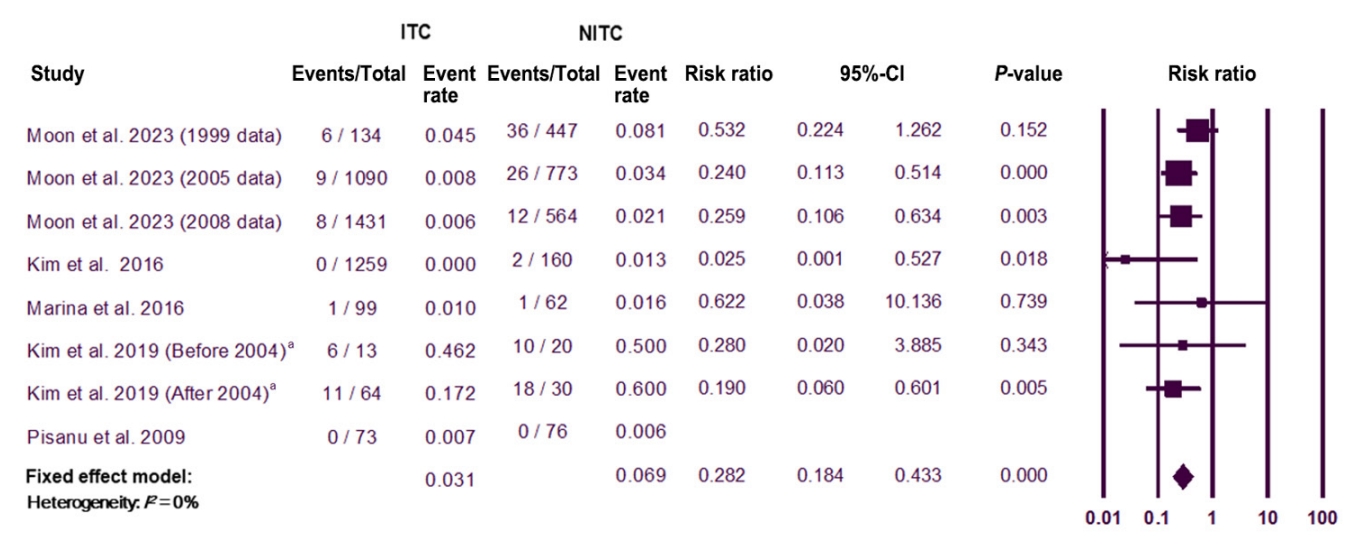
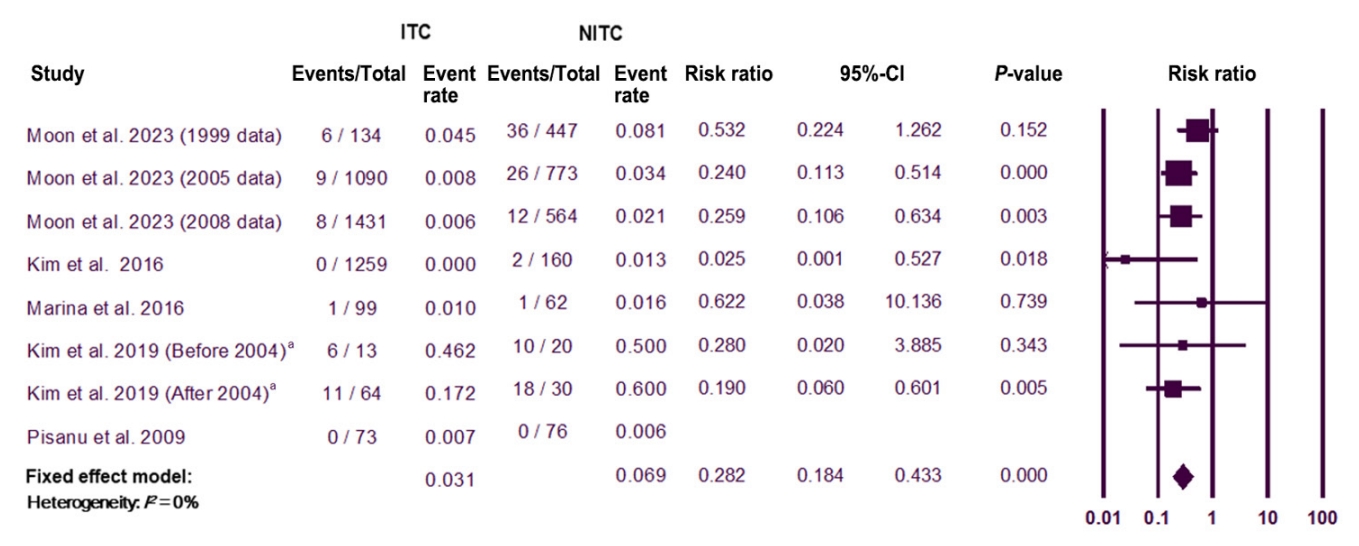
- Five studies with eight datasets were included in the meta-analysis of thyroid cancer-specific mortality. In comparison with the NITC group, the ITC group had a lower risk of thyroid cancer-specific mortality (OR, 0.28; 95% CI, 0.18 to 0.43) (Fig. 5). Heterogeneity was not significant among these studies (I2=0%). The funnel plot analysis and the Egger test revealed no significant publication bias (P=0.503) (Supplemental Fig. S1). The sensitivity analysis showed robust results from repeated analyses after excluding each study (Supplemental Fig. 2).
- Regarding postoperative complications, only two articles were included, which was insufficient to perform a meta-analysis. A summary derived from systematic reviews is presented in Supplemental Table S4, revealing no significant differences in the prevalence of postoperative complications between ITC and NITC.
RESULTS
- This meta-analysis demonstrated that ITC patients had lower risks of unfavorable clinicopathologic characteristics, such as aggressive histology, large tumor size, ETE, lymph node metastasis, distant metastasis, and advanced TNM stage, than NITC patients. Furthermore, in ITC patients, the risks of recurrence and mortality were significantly lower than in NITC patients, confirming the effectiveness and benefits of thyroid cancer screening.
- In the 2017 USPSTF report [5], there was insufficient evidence to conclude whether thyroid cancer screening for adults leads to a reduced risk of thyroid cancer-specific morbidity, mortality, and/or all-cause mortality. Recently, Chooi et al. [10] reported a systematic review on the prognosis of thyroid incidentalomas. Although a meta-analysis could not be performed for the prognosis due to heterogeneity in the inclusion criteria, prognosis marker assessments, and follow-up duration, they reviewed 14 studies on the prognosis or various prognostic markers, such as histological characteristics and cancer staging in ITC and NITC. Four studies on recurrence—not mortality—were included to compare the thyroid cancer prognosis of ITC and NITC. All included studies showed a lower risk of recurrence in ITC than in NITC [11,12,22,25], although some studies did not reach statistical significance. Meanwhile, in our study, we added more studies through a thorough systematic review and performed a meta-analysis with recent studies, including the National Epidemiological Survey of Thyroid cancer (NEST) [21].
- We analyzed the NEST study [21] as three separate populations according to the time period, because the study randomly sampled Korean thyroid cancer patients at three time points (1999, 2005, and 2008) [26]. As Kim et al. [18] described previously, the early detection of thyroid cancer by ultrasound in Korea started in earnest in 2004 [27]. Moreover, the incidence of thyroid cancer increased dramatically in 2009 [28]. Therefore, to reflect heterogeneity in the clinicopathological features of thyroid cancer over time, each population from these three time points was analyzed as an independent group in this study.
- The increased incidence of thyroid cancer coincided with the introduction and widespread use of imaging modalities such as ultrasound, and the improved sensitivity of diagnostic tools since the 2000s [4,29]. Despite the rising incidence of thyroid cancer, mortality from thyroid cancer remained stable, which has been interpreted as reflecting overdiagnosis [30,31]. However, according to a recent study of Surveillance, Epidemiology, and End Results (SEER) data, thyroid cancer incidence decreased during 2014 to 2018, but incidence-based mortality continued to increase [32]. Given the results of our study, which showed that thyroid cancer screening can reduce mortality, overdiagnosis alone might not be sufficient to explain the increased incidence of thyroid cancer.
- The current meta-analysis revealed that patients with ITC had more indolent tumor behaviors and better prognoses, suggesting that early detection improves the clinical outcomes of thyroid cancer. For patients with locally advanced or high-risk thyroid cancer, early diagnosis and treatment can prevent serious disease progression [33]. Therefore, to solve the issues of overdiagnosis and overtreatment caused by thyroid cancer screening, it is necessary to minimize the harms of screening and treatment while maintaining the benefits of screening. Moreover, it is critical to develop appropriate diagnosis and management guidelines for incidentally detected thyroid nodules. In this context, the Korean Society of Thyroid Radiology revised the indications for fine-needle aspiration to be stricter [34,35] to reduce unnecessary diagnostic tests. In addition, active surveillance for low-risk thyroid cancers has been introduced [36] and large-scale multicenter prospective clinical studies are currently being conducted in Korea, thereby minimizing the risk of unnecessary surgery [37,38].
- Our study has several strengths. First, this is the first meta-analysis to comprehensively compare the clinicopathological characteristics and prognosis of ITC and NITC. Second, we demonstrated that ITC had better thyroid cancer-specific survival. The ultimate goal of cancer screening, which generally aims to detect cancer at an early stage rather than to prevent cancer occurrence, is to reduce cancer-related mortality [39,40]. Thus, it is meaningful that this study revealed a survival benefit, reflecting the purpose of cancer screening. However, this study has certain limitations. First, the spectrum of ITC was wide, including incidentalomas detected by various imaging modalities (ultrasound, carotid Doppler, neck CT/MRI, and 18F-FDG PET/CT) or occult tumors found in the surgical pathology specimens of benign tumors. Furthermore, NITC covered various symptoms or signs, mostly neck symptoms, but one study [18] included patients with systemic symptoms due to distant metastasis in the NITC category. Second, no prospective randomized clinical trials were included in the meta-analysis, and retrospective cohort studies harbor a high probability of bias, as is widely recognized [41,42]. Nevertheless, the included studies were assessed as having a low-risk of bias, considering the large number of participants and well-controlled design.
- In conclusion, our findings provide important evidence for a survival benefit from the early detection of thyroid cancer compared to symptomatic thyroid cancer.
DISCUSSION
Supplementary Material
Supplementary Table S4.
Supplementary Fig. S1.
Supplementary Fig. S2.
Supplementary Fig. S3.
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conception or design: E.K.L., Y.J.P. Acquisition, analysis, or interpretation of data: S.M., Y.S.S., K.Y.J., E.K.L. Drafting the work or revising: S.M., Y.S.S., K.Y.J., E.K.L. Final approval of the manuscript: S.M., Y.S.S., K.Y.J., E.K.L., Y.J.P.
Article information
-
Acknowledgements
- This study was supported by the Korean Thyroid Association, research funding from the National Cancer Center (Grant Number 2210521-2 and 2112570-3), and a grant from the National Research Foundation (NRF) of Korea (NRF-2020R1C1-C1003924).
- We acknowledge and thank Miyoung Choi (National Evidence-based Healthcare Collaborating Agency, Division of Health Technology Assessment Research) and Chang Hee Cho (The Korean Society of Radiology), who contributed to searching and interpreting the evidence.

| Study | Country, recruitment years | Groupa | Method of incidental detection | No. of patients | Mean age, yr | PTC, % | Mean tumor size, cm | Lymph node metastasis at diagnosis % | Distant metastasis at diagnosis % | No. of recurrence (%) | No. of thyroid cancerspecific death (%) | Overall follow-up, mo (range) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Moon et al. (2023) [21] | Korea, 1999, 2005, 2008 | ITC | Imaging | 2,655 | 46.8 | 95.3 | 1.0 | 42 | 0.6 | NR | 23 (0.9) | 164 | |
| NITC | 1,784 | 47.0 | 92.7 | 1.7 | 46.8 | 1 | NR | 74 (4.1) | 179 | ||||
| Solis-Pazmino et al. (2021) [22] | Ecuador, 2014–2017 | ITC | Imaging, pathology | 246 | 46.3 | NR | 2.23 | 43.8 | NR | NR | NR | NR | |
| NITC | 206 | 43 | NR | 3.57 | 53.7 | NR | NR | NR | NR | ||||
| Kim et al. (2019) [18] | Korea, 1994–2013 | Before 2004 | Imaging, pathology | 33 | 44.2 | 54.5 | 3.5 | 51.5 | 100 | NR | 16 (48.5) | 72 (0–276) | |
| ITC | 13 | 100 | NR | 6 (46.2) | |||||||||
| NITCb | 20 | 100 | NR | 10 (50.0) | |||||||||
| After 2004 | 94 | 50.7 | 52.1 | 3.7 | 64.5 | 100 | NR | 29 (30.9) | 72 (0–276) | ||||
| ITC | 64 | 100 | NR | 11 (17.2) | |||||||||
| NITCb | 30 | 100 | NR | 18 (60.0) | |||||||||
| Shakil et al. (2017) [11] | USA, 2005–2014 | ITC | Imaging, pathology | 46 | 53.0 | 95.5 | NR | 13 | NR | 3 (6.7)d | NR | 27.0 (6–55) | |
| NITC | 126 | 45.3 | 94.4 | NR | 29.4 | NR | 25 (20.8)d | NR | 26.5 (6–58) | ||||
| Marina et al. (2017) [13] | Italy, 1998–2015 | ITC | Imaging | 99 | 50.0 | 92.9 | 1.3 | 13.3 | 1.0 | 4 (4) | 1 (1.0) | 67.2 (32.4–114) | |
| NITC | 62 | 44.0 | 87.1 | 2.5 | 23.3 | 6.5 | 7 (11) | 1 (1.6) | 67.2 (32.4–114) | ||||
| Farra et al. (2017) [23] | USA, 2010–2016 | ITC | Imaging | 65 | 54 | 91 | NR | 47 | NR | NR | NR | NR | |
| NITC | 401 | 50 | 92 | NR | 33 | NR | NR | NR | NR | ||||
| Kim et al. (2016) [12] | Korea, 2006–2009 | ITC | Imaging | 1,259 | 55.0 | 100 | 0.9 | 40.2 | 0 | 41 (3.3) | 0 | 95.0 (24–119) | |
| NITC | 160 | 55.0 | 100 | 1.1 | 52.5 | 1.9 | 17 (10.6) | 2 (1.3) | 96.0 (24–118) | ||||
| Brito et al. (2015) [17] | USA, 2000–2012 | 1935–1999 | Imaging, pathology | ||||||||||
| ITC | 59 | 52.3 | 89.8 | 0.98 | NR | NR | NR | NR | NR | ||||
| NITC | 203 | 44.2 | 79.8 | 2.3 | NR | NR | NR | NR | NR | ||||
| 2000–2012 | |||||||||||||
| ITC | 113 | 49.6 | 95.6 | 1.3 | NR | NR | NR | NR | NR | ||||
| NITC | 100 | 42.7 | 91 | 2.3 | NR | NR | NR | NR | NR | ||||
| Malone et al. (2014) [15] | USA, 2007–2010 | ITC | Imaging | 184 | 51 | NR | 1.6 | 39 | NR | NR | NR | NR | |
| NITC | 218 | 46 | NR | 2.1 | 58 | NR | NR | NR | NR | ||||
| Bahl et al. (2014) [16] | USA, 2003–2012 | ITC | Imaging | 101 | 57 | 84.2 | 1.8 | 24.7 | 0 | NR | NR | NR | |
| NITC | 485 | 46 | 82.7 | 2.2 | 32.4 | 1.0 | NR | NR | NR | ||||
| Yoo et al. (2013) [24] | USA, 2008–2009 | ITC | Imaging | 31 | 56.4 | 83.9 | 2.15 | 22.6 | 0 | NR | NR | NR | |
| NITC | 207 | 41.8 | 87.9 | 2.11 | 20.8 | 0.5 | NR | NR | NR | ||||
| Pisanu et al. (2009) [14] | Italy, 1998–2007 | ITC | Pathology | 73 | 52.5 | 100 | 0.4 | 1.4 | NR | 0 | 0 | 65.2 | |
| NITC | 76 | 49.5 | 100 | 0.7 | 34.1 | NR | 3 (3.9) | 0 | 65.2 | ||||
| Choi et al. (2008) [20] | Korea, 2006–2008 | ITC | Imaging | 46 | 51.1 | 93.5 | 0.6 | 28.3 | NR | NR | NR | NR | |
| NITC | 157 | 48.1 | 97.5 | 1.6 | 29.9 | NR | NR | NR | NR | ||||
| Chung et al. (2001) [19] | Korea, 1997–1998 | ITCc | Imaging | 37 | 46.5 | 97.3 | 1.0 | 40.5 | NR | NR | NR | NR | |
| NITC | 106 | 45.3 | 92.5 | 1.9 | 78.3 | NR | NR | NR | NR | ||||
PTC, papillary thyroid carcinoma; ITC, incidental thyroid cancer; NR, not reported; NITC, non-incidental thyroid cancer.
a Incidental thyroid cancer was defined as an unexpected thyroid cancer incidentally detected by imaging methods (ultrasound, computed tomography/magnetic resonance imaging, and 18-fludeoxyglucose positron emission tomography/computed tomography) or analysis of a surgical pathology specimen. Non-incidental thyroid cancer was defined as thyroid cancer that had been detected due to clinical signs or symptoms (palpable thyroid lump, voice change or difficulty in swallowing, abnormality on physical examination by a physician, and so on);
b The enrolled patients had thyroid cancer with initial distant metastasis. The NITC group included both patients with local symptoms and patients with systemic symptoms;
c Women who were scheduled to undergo either a breast cancer screening or a follow-up examination for breast cancer were screened for thyroid cancer;
d Recurrence or residual.
- 1. Kim J, Gosnell JE, Roman SA. Geographic influences in the global rise of thyroid cancer. Nat Rev Endocrinol 2020;16:17–29.ArticlePubMedPDF
- 2. Davies L, Welch HG. Increasing incidence of thyroid cancer in the United States, 1973-2002. JAMA 2006;295:2164–7.ArticlePubMed
- 3. Pizzato M, Li M, Vignat J, Laversanne M, Singh D, La Vecchia C, et al. The epidemiological landscape of thyroid cancer worldwide: GLOBOCAN estimates for incidence and mortality rates in 2020. Lancet Diabetes Endocrinol 2022;10:264–72.ArticlePubMed
- 4. Li M, Dal Maso L, Vaccarella S. Global trends in thyroid cancer incidence and the impact of overdiagnosis. Lancet Diabetes Endocrinol 2020;8:468–70.ArticlePubMed
- 5. Lin JS, Bowles EJ, Williams SB, Morrison CC. Screening for thyroid cancer: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA 2017;317:1888–903.ArticlePubMed
- 6. Yi KH, Kim SY, Kim DH, Kim SW, Na DG, Lee YJ, et al. The Korean guideline for thyroid cancer screening. J Korean Med Assoc 2015;58:302–12.Article
- 7. US Preventive Services Task Force, Bibbins-Domingo K, Grossman DC, Curry SJ, Barry MJ, Davidson KW, et al. Screening for thyroid cancer: US Preventive Services Task Force recommendation statement. JAMA 2017;317:1882–7.ArticlePubMed
- 8. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 2009;339:b2535.ArticlePubMedPMC
- 9. National Evidence-based Healthcare Collaborating Agency. Effectiveness of ultrasonographic screening for thyroid cancer 2012 [Internet]. Seoul: NECA; 2023 [cited 2023 Feb 17]. Available from: https://neca.re.kr.
- 10. Chooi JE, Ravindiran A, Balasubramanian SP. The influence of incidental detection of thyroid nodule on thyroid cancer risk and prognosis: a systematic review. Clin Endocrinol (Oxf) 2022;96:246–54.ArticlePubMedPDF
- 11. Shakil J, Ansari MZ, Brady J, Xu J, Robbins RJ. Lower rates of residual/recurrent disease in patients with incidentally discovered thyroid carcinoma. Endocr Pract 2017;23:163–9.ArticlePubMed
- 12. Kim SH, Roh JL, Gong G, Cho KJ, Choi SH, Nam SY, et al. Differences in the recurrence and survival of patients with symptomatic and asymptomatic papillary thyroid carcinoma: an observational study of 11,265 person-years of follow-up. Thyroid 2016;26:1472–9.ArticlePubMed
- 13. Marina M, Ceda GP, Aldigeri R, Ceresini G. Causes of referral to the first endocrine visit of patients with thyroid carcinoma in a mildly iodine-deficient area. Endocrine 2017;57:247–55.ArticlePubMedPDF
- 14. Pisanu A, Reccia I, Nardello O, Uccheddu A. Risk factors for nodal metastasis and recurrence among patients with papillary thyroid microcarcinoma: differences in clinical relevance between nonincidental and incidental tumors. World J Surg 2009;33:460–8.ArticlePubMedPDF
- 15. Malone MK, Zagzag J, Ogilvie JB, Patel KN, Heller KS. Thyroid cancers detected by imaging are not necessarily small or early stage. Thyroid 2014;24:314–8.ArticlePubMed
- 16. Bahl M, Sosa JA, Nelson RC, Esclamado RM, Choudhury KR, Hoang JK. Trends in incidentally identified thyroid cancers over a decade: a retrospective analysis of 2,090 surgical patients. World J Surg 2014;38:1312–7.ArticlePubMedPDF
- 17. Brito JP, Al Nofal A, Montori VM, Hay ID, Morris JC. The impact of subclinical disease and mechanism of detection on the rise in thyroid cancer incidence: a population-based study in Olmsted County, Minnesota during 1935 through 2012. Thyroid 2015;25:999–1007.ArticlePubMedPMC
- 18. Kim H, Park SY, Jung J, Kim JH, Hahn SY, Shin JH, et al. Improved survival after early detection of asymptomatic distant metastasis in patients with thyroid cancer. Sci Rep 2019;9:18745.ArticlePubMedPMCPDF
- 19. Chung WY, Chang HS, Kim EK, Park CS. Ultrasonographic mass screening for thyroid carcinoma: a study in women scheduled to undergo a breast examination. Surg Today 2001;31:763–7.ArticlePubMedPDF
- 20. Choi YJ, Park YL, Koh JH. Prevalence of thyroid cancer at a medical screening center: pathological features of screen-detected thyroid carcinomas. Yonsei Med J 2008;49:748–56.ArticlePubMedPMC
- 21. Moon S, Lee EK, Choi H, Park SK, Park YJ. Survival comparison of incidentally found versus clinically detected thyroid cancers: an analysis of a nationwide cohort study. Endocrinol Metab (Seoul) 2023;38:81–92.ArticlePubMedPMCPDF
- 22. Solis-Pazmino P, Salazar-Vega J, Lincango-Naranjo E, Garcia C, Koupermann GJ, Ortiz-Prado E, et al. Thyroid cancer overdiagnosis and overtreatment: a cross-sectional study at a thyroid cancer referral center in Ecuador. BMC Cancer 2021;21:42.ArticlePubMedPMCPDF
- 23. Farra JC, Picado O, Liu S, Ouyang W, Teo R, Franco AM, et al. Clinically significant cancer rates in incidentally discovered thyroid nodules by routine imaging. J Surg Res 2017;219:341–6.ArticlePubMed
- 24. Yoo F, Chaikhoutdinov I, Mitzner R, Liao J, Goldenberg D. Characteristics of incidentally discovered thyroid cancer. JAMA Otolaryngol Head Neck Surg 2013;139:1181–6.ArticlePubMed
- 25. Marina M, Serra MF, Aldigeri R, Ceresini G. Incidental versus clinically diagnosed differentiated thyroid cancer in both adult and elderly subjects: histological characteristics and follow-up in a retrospective analysis from a single institution. Endocrine 2020;68:584–91.ArticlePubMedPDF
- 26. Oh CM, Kong HJ, Kim E, Kim H, Jung KW, Park S, et al. National epidemiologic survey of thyroid cancer (NEST) in Korea. Epidemiol Health 2018;40:e2018052.ArticlePubMedPMC
- 27. Park S, Oh CM, Cho H, Lee JY, Jung KW, Jun JK, et al. Association between screening and the thyroid cancer “epidemic” in South Korea: evidence from a nationwide study. BMJ 2016;355:i5745.ArticlePubMedPMC
- 28. Jung KW, Won YJ, Kong HJ, Oh CM, Cho H, Lee DH, et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2012. Cancer Res Treat 2015;47:127–41.ArticlePubMedPMCPDF
- 29. Ahn HS, Kim HJ, Welch HG. Korea’s thyroid-cancer “epidemic”: screening and overdiagnosis. N Engl J Med 2014;371:1765–7.ArticlePubMed
- 30. Vaccarella S, Franceschi S, Bray F, Wild CP, Plummer M, Dal Maso L. Worldwide thyroid-cancer epidemic?: the increasing impact of overdiagnosis. N Engl J Med 2016;375:614–7.ArticlePubMed
- 31. Franceschi S, Vaccarella S. Thyroid cancer: an epidemic of disease or an epidemic of diagnosis? Int J Cancer 2015;136:2738–9.ArticlePubMed
- 32. Megwalu UC, Moon PK. Thyroid cancer incidence and mortality trends in the United States: 2000-2018. Thyroid 2022;32:560–70.ArticlePubMed
- 33. Nguyen QT, Lee EJ, Huang MG, Park YI, Khullar A, Plodkowski RA. Diagnosis and treatment of patients with thyroid cancer. Am Health Drug Benefits 2015;8:30–40.
- 34. Shin JH, Baek JH, Chung J, Ha EJ, Kim JH, Lee YH, et al. Ultrasonography diagnosis and imaging-based management of thyroid nodules: revised Korean Society of Thyroid Radiology consensus statement and recommendations. Korean J Radiol 2016;17:370–95.ArticlePubMedPMCPDF
- 35. Ha EJ, Chung SR, Na DG, Ahn HS, Chung J, Lee JY, et al. 2021 Korean thyroid imaging reporting and data system and imaging-based management of thyroid nodules: Korean Society of Thyroid Radiology consensus statement and recommendations. Korean J Radiol 2021;22:2094–123.ArticlePubMedPMCPDF
- 36. Yi KH, Lee EK, Kang HC, Koh Y, Kim SW, Kim IJ, et al. 2016 Revised Korean Thyroid Association management guidelines for patients with thyroid nodules and thyroid cancer. Int J Thyroidol 2016;9:59–126.ArticlePDF
- 37. Moon JH, Kim JH, Lee EK, Lee KE, Kong SH, Kim YK, et al. Study protocol of multicenter prospective cohort study of active surveillance on papillary thyroid microcarcinoma (MAeSTro). Endocrinol Metab (Seoul) 2018;33:278–86.ArticlePubMedPMCPDF
- 38. Jeon MJ, Kang YE, Moon JH, Lim DJ, Lee CY, Lee YS, et al. Protocol for a Korean multicenter prospective cohort study of active surveillance or surgery (KoMPASS) in papillary thyroid microcarcinoma. Endocrinol Metab (Seoul) 2021;36:359–64.ArticlePubMedPMCPDF
- 39. Prorok PC. Epidemiologic approach for cancer screening: problems in design and analysis of trials. Am J Pediatr Hematol Oncol 1992;14:117–28.PubMed
- 40. Kramer BS, Brawley OW. Cancer screening. Hematol Oncol Clin North Am 2000;14:831–48.ArticlePubMed
- 41. Carlson MD, Morrison RS. Study design, precision, and validity in observational studies. J Palliat Med 2009;12:77–82.ArticlePubMedPMC
- 42. Boyko EJ. Observational research: opportunities and limitations. J Diabetes Complications 2013;27:642–8.ArticlePubMedPMC
References
Figure & Data
References
Citations
- To Screen or Not to Screen?
Do Joon Park
Endocrinology and Metabolism.2023; 38(1): 69. CrossRef - The 2017 United States Preventive Services Task Force Recommendation for Thyroid Cancer Screening Is No Longer the Gold Standard
Ka Hee Yi
Endocrinology and Metabolism.2023; 38(1): 72. CrossRef - Thyroid Cancer Screening: How to Maximize Its Benefits and Minimize Its Harms
Jung Hwan Baek
Endocrinology and Metabolism.2023; 38(1): 75. CrossRef - Delayed Surgery for and Outcomes of Papillary Thyroid Cancer: Is the Pendulum Still Swinging?
Giorgio Grani
Clinical Thyroidology.2023; 35(5): 192. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite