Articles
- Page Path
- HOME > Endocrinol Metab > Volume 37(4); 2022 > Article
-
Original ArticleThyroid Frequency of TERT Promoter Mutations in Real-World Analysis of 2,092 Thyroid Carcinoma Patients
 Keypoint
Keypoint
Telomerase reverse transcriptase (TERT) promoter mutations are associated with increased recurrence and mortality in patients with thyroid carcinoma. This study included 2,092 patients with thyroid carcinoma who underwent thyroid surgery and found that the frequency of TERT promoter mutations was significantly associated with older age at diagnosis, larger primary tumor size, and aggressive histological type. -
Heera Yang1*
 , Hyunju Park1*, Hyun Jin Ryu1, Jung Heo1, Jung-Sun Kim2, Young Lyun Oh2, Jun-Ho Choe3, Jung Han Kim3, Jee Soo Kim3, Hye Won Jang4, Tae Hyuk Kim1, Sun Wook Kim1, Jae Hoon Chung1
, Hyunju Park1*, Hyun Jin Ryu1, Jung Heo1, Jung-Sun Kim2, Young Lyun Oh2, Jun-Ho Choe3, Jung Han Kim3, Jee Soo Kim3, Hye Won Jang4, Tae Hyuk Kim1, Sun Wook Kim1, Jae Hoon Chung1 -
Endocrinology and Metabolism 2022;37(4):652-663.
DOI: https://doi.org/10.3803/EnM.2022.1477
Published online: July 22, 2022
1Division of Endocrinology and Metabolism, Department of Medicine, Thyroid Center, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
2Department of Pathology and Translational Genomics, Sungkyunkwan University School of Medicine, Seoul, Korea
3Division of Breast and Endocrine Surgery, Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
4Department of Medical Education, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- Corresponding author: Jae Hoon Chung. Division of Endocrinology and Metabolism, Department of Medicine, Thyroid Center, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 06351, Korea Tel: +82-2-3410-3434, Fax: +82-2-3410-3849, E-mail: thyroid@skku.edu
- *These authors contributed equally to this work.
Copyright © 2022 Korean Endocrine Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- Telomerase reverse transcriptase (TERT) promoter mutations are associated with increased recurrence and mortality in patients with thyroid carcinoma. Previous studies on TERT promoter mutations were retrospectively conducted on a limited number of patients.
-
Methods
- We prospectively collected data on all consecutive patients who underwent thyroid carcinoma surgery between January 2019 and December 2020 at the Samsung Medical Center, Seoul, Korea. We included 2,092 patients with thyroid carcinoma.
-
Results
- Of 2,092 patients, 72 patients (3.4%) had TERT promoter mutations. However, the frequency of TERT promoter mutations was 0.5% in papillary thyroid microcarcinoma (PTMC) ≤1 cm and it was 5.8% in papillary thyroid carcinoma (PTC) >1 cm. The frequency of TERT promoter mutations was significantly associated with older age at diagnosis (odds ratio [OR], 1.12; P<0.001), larger primary tumor size (OR, 2.02; P<0.001), and aggressive histological type (OR, 7.78 in follicular thyroid carcinoma; OR, 10.33 in poorly differentiated thyroid carcinoma; OR, 45.92 in anaplastic thyroid carcinoma; P<0.001). Advanced T stage, advanced N stage, and distant metastasis at diagnosis were highly prevalent in mutated thyroid cancers. However, initial distant metastasis was not present in patients with TERT promoter mutations in PTMC. Although the C228T mutation was more highly detected than the C250T mutation (64 cases vs. 7 cases), there were no significant clinicopathological differences.
-
Conclusion
- This study is the first attempt to investigate the frequency of TERT promoter mutations in a real-world setting. The frequency of TERT promoter mutations in PTC was lower than expected, and in PTMC, young patients, and female patients, the frequency was very low.
- The incidence of thyroid carcinoma has increased with time, but there has been no increase in mortality rate [1-3]. Most patients with thyroid carcinoma have a long survival. Therefore, it is important to distinguish patients who need aggressive treatment from those who do not. Conventional prognostic factors cannot predict the outcome of each patient completely [4-6]. Therefore, more precise factors for estimating the oncologic outcome are required to select a proper therapeutic strategy for each patient.
- Telomerase reverse transcriptase (TERT) promoter mutations are the main genetic alteration in the risk stratification of thyroid carcinoma. TERT promoter mutations increase telomerase activity, which protects telomeres from shortening and allows carcinoma cells to undergo immortalization. The TERT promoter mutations have been reported to be highly prevalent in tumors with aggressive or dedifferentiated histology [7-9], and it is associated with increased recurrence and mortality in patients with thyroid carcinoma [7,10-14]. Our team reported that TERT promoter mutations can be a molecular prognostic marker, and may improve the prediction of a prognosis when merged with the conventional staging system in differentiated thyroid carcinoma (DTC) [15-17].
- Although it is well known that TERT promoter mutations are significant factors in oncologic outcomes, the real-world frequency of TERT promoter mutations is unclear. Previous studies on TERT promoter mutations were retrospectively conducted on limited subjects and did not reflect the actual situation in the clinical setting. The studies may overestimate the frequency of TERT promoter mutations because of potential selection bias. In this study, we prospectively performed TERT promoter mutation tests in all consecutive patients who underwent surgery for thyroid carcinoma in our institution. Therefore, this study can provide real-world data on TERT promoter mutation frequency.
INTRODUCTION
- Patients and clinicopathological data
- We collected data from 2,143 consecutive patients with thyroid tumors who underwent thyroidectomy or neck dissection between January 2019 and December 2020 at the Samsung Medical Center, Seoul, Korea. The TERT promoter mutation test was performed immediately after surgery regardless of individual clinical risks. Among the 2,143 patients, nine patients were pathologically diagnosed with medullary thyroid carcinoma and 42 patients who were suspected of malignancy in preoperative fine-needle aspiration or core-needle biopsy were diagnosed with benign disease (follicular adenoma, Hurthle cell adenoma, well-differentiated tumor of uncertain malignant potential, and follicular tumor of uncertain malignant potential) after surgery were excluded. Finally, 2,092 thyroid carcinoma patients were included in the study. We defined papillary thyroid microcarcinoma (PTMC) as a primary tumor size ≤1 cm.
- The clinical information of patients was obtained from electronic medical records. Cancer staging was conducted by using the 8th edition of the American Joint Committee on Cancer (AJCC) staging system. The Institutional Review Board at the Samsung Medical Center approved this study (IRB 2022-01-072). Patient consent was waived by the committee because of the retrospective chart review study design and the use of only deidentified clinicopathologic information.
- Detection of TERT promoter mutations
- Genomic DNA was extracted from formalin-fixed paraffin-embedded (FFPE) tissue using a Qiagen DNA FFPE Tissue Kit (Qiagen, Venlo, Netherlands) according to the manufacturer’s instructions. Polymerase chain reaction (PCR) sequencing was carried out to identify TERT promoter mutations using an iTERT mutation detection kit (Geninus Inc., Seoul, Korea). The PCR reactions were assembled on ice and preincubated at 94°C for 15 minutes, followed by 40 cycles at 94°C for 20 seconds, 58°C for 40 seconds, 72°C for 1 minute, and a final extension at 72°C for 5 minutes using a C1000 Touch Thermal Cycler Kit (Bio-Rad, Hercules, CA, USA). Bidirectional sequencing was performed using a BigDye Terminator v.3.1 Kit (Applied Biosystems, Foster City, CA, USA) on an ABI 3130xL Genetic Analyzer. The sample was considered mutation-positive if mutations were detected in both the forward and reverse DNA strands.
- Statistical analysis
- Continuous variables are presented as mean±standard deviation (SD), and categorical variables are presented as numbers and percentages. Student’s t test was performed for the comparison of continuous variables, and the chi-square test or Fisher’s exact test was performed for the comparison of categorical variables as appropriate. P values were two-sided, and P values less than 0.05 were considered statistically significant. Linear by linear association was used to analyze P for trend, age, and primary tumor size. Univariate logistic regression was used to evaluate the association between TERT promoter mutations and clinicopathological variables. Statistical analysis was performed using SPSS version 25.0 for Windows (IBM Corp., Armonk, NY, USA).
METHODS
- Baseline characteristics
- The detailed clinicopathological data of 2,092 patients with thyroid carcinoma are presented in Table 1. The mean±SD age was 45.6±13.0 years, and the group included 1,539 (73.6%) females. The mean±SD tumor size was 1.33±1.14 cm. Most patients (96.6%) had papillary thyroid carcinoma (PTC), 38 (1.8%) patients had follicular thyroid carcinoma (FTC), 14 (0.7%) patients had Hurthle cell thyroid carcinoma (HTC), 13 (0.6%) patients had poorly differentiated thyroid carcinoma (PDTC), and seven (0.3%) patients had anaplastic thyroid carcinoma (ATC). According to the 8th edition of the AJCC staging system, 1,671 (79.9%) patients had T1 stage, 204 (9.8%) had T2 stage, 175 (8.4%) had T3 stage, and 42 (2.0%) had T4 stage. The proportion of N0 was 771 (36.9%), N1a was 669 (32.0%), and N1b was 292 (14.0%). Distant metastasis at the time of diagnosis was found in 32 (1.5%) patients. Out of 72 patients with TERT promoter mutations, 64 had a TERT promoter mutation at hotspot C228T (chr5: 1,295,228C>T), seven patients had the C250T (chr5: 1,295,250C>T) mutation, and one patient had the C228A (chr5: 1,295,228C>A) mutation.
- Comparison of clinicopathological characteristics of patients with TERT promoter mutations to patients with wild-type
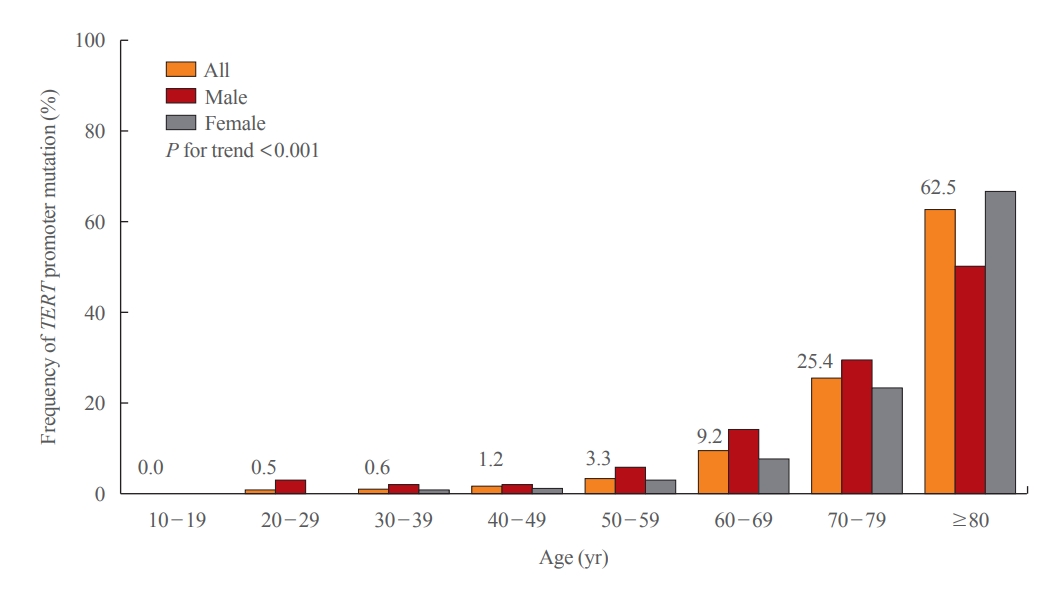
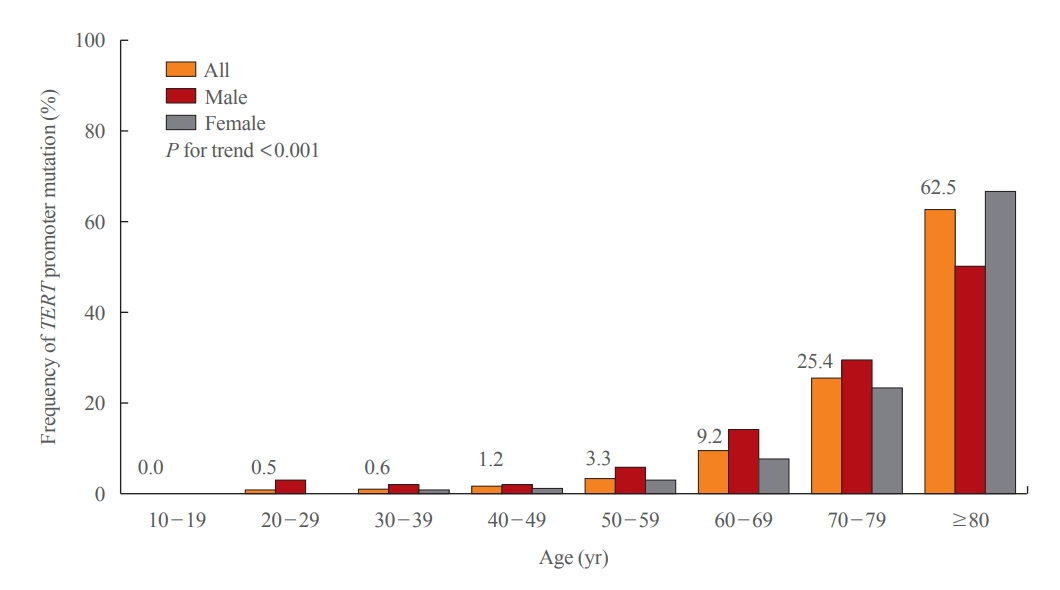
- The clinicopathological comparison of patients with TERT promoter mutations to those with wild-type are shown in Table 2. The mean±SD age of the 72 patients with TERT promoter mutations was 62.5±12.9 years. The frequency of TERT promoter mutations increased significantly with age (odds ratio [OR], 1.13; P<0.001), and it was significantly higher in males compared with females (OR, 2.22; P=0.003). This significance was consistent when patients were classified according to the age at diagnosis. TERT promoter mutations were not found in patients under the age of 19, but it was detected in 0.5% of patients 20 to 29 years old, 0.6% of patients 30 to 39 years old, 1.2% of patients 40 to 49 years old, 3.3% of patients 50 to 59 years old, 9.2% of patients 60 to 69 years old, 25.4% of patients 70 to 79 years old, and 62.5% of patients 80 years and older (P for trend <0.001) (Fig. 1). In particular, the proportion of TERT promoter mutations reached 0.9% in female patients aged under 49 years.
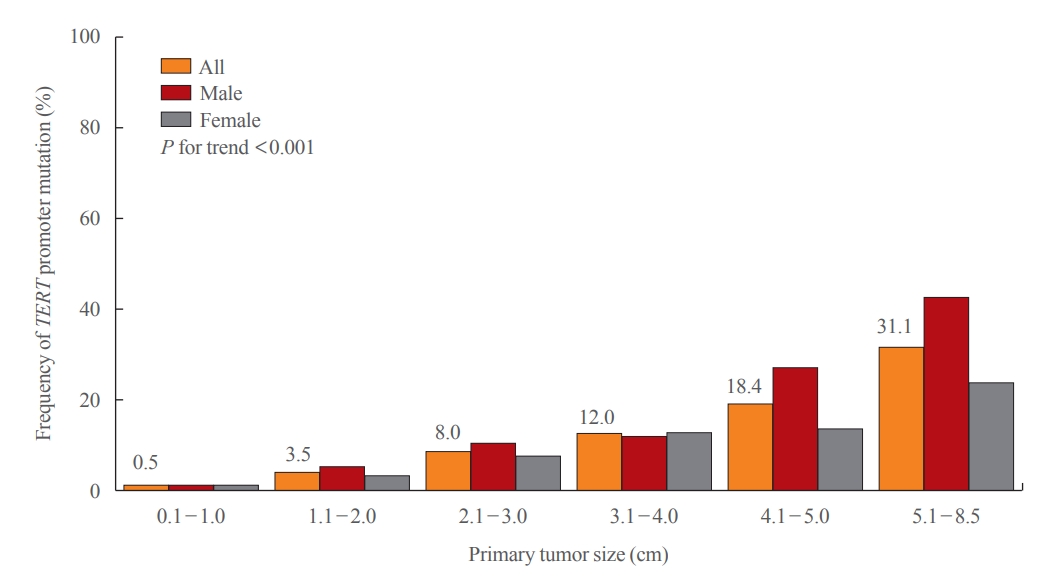
- The primary tumor size in the patients with TERT promoter mutations was significantly larger than in those with wild-type (OR, 2.02; P<0.001). This significance was consistent when patients were classified according to the primary tumor size. The frequency of TERT promoter mutations increased significantly as the tumor size increased (P for trend <0.001) (Fig. 2). TERT promoter mutations were found in 0.5% of tumors less than 1 cm in size, 3.5% of tumors 1.1 to 2.0 cm, 8.0% of tumors 2.1 to 3.0 cm, 12.0% of tumors 3.1 to 4.0 cm, 18.4% of tumors 4.1 to 5.0 cm, and 31.1% of tumors more than 5.1 cm. The increase in mutations as the tumor size increased was more prominent in men than in women.
- The frequency of TERT promoter mutations significantly differed among the histological type. FTC, PDTC, and ATC had significantly higher TERT promoter mutations than PTC ([OR, 7.78; P<0.001], [OR, 10.33; P<0.001], and [OR, 45.92; P<0.001], respectively). In PTC, TERT promoter mutations were detected in 2.5% of classic PTC, 7.6% of tall cell variant PTC or classic with tall cell feature PTC, and 33.3% of solid variant PTC. TERT promoter mutations were not detected in cribriform-morular variant PTC, diffuse sclerosing variant PTC, Hobnail variant PTC, oncocytic variant PTC, and Warthin-like variant PTC (Supplemental Table S1). In FTC, TERT promoter mutations were detected in 9.7% of minimally invasive FTC, 40% of encapsulated angioinvasive FTC, and 100% of widely invasive FTC (Supplemental Table S2).
- Advanced T stage and N stage were also significantly associated with TERT promoter mutations. The frequency of distant metastasis at the time of diagnosis was significantly higher in patients with TERT promoter mutations. The significance of the association between the TERT promoter mutational status and conventional clinicopathological variables were consistent when analyzed only in PTC patients (Supplemental Table S3, Supplemental Figs. S1, S2).
- Association of TERT promoter mutation status according to primary tumor size and age at diagnosis in PTC
- The patients with PTC, the largest subgroup, were categorized into two groups based on primary tumor size. The frequency of TERT promoter mutations in PTMC was 0.52%, and 5.8% in PTC >1 cm (Table 3). In the PTMC group, age (categorical), sex, and presence of initial distant metastasis were not significantly different. In six patients with TERT promoter mutations, one patient had recurrent laryngeal nerve invasion (T4) and three patients had lymph node metastasis; one patient was N1a, and two patients were N1b. Hence, the clinicopathological characteristics of PTC patients were similar in the entire cohort.
- We also compared clinicopathological characteristics according to age at diagnosis in PTC (Table 4). The frequency of TERT promoter mutations in age <55 years was 0.80%, and 9.8% in age ≥55 years. Age at diagnosis was significantly older in patients with TERT promoter mutations in both groups.
- Comparison of clinicopathological characteristics between C228T and C250T mutations
- Out of 72 patients with TERT promoter mutation, 64 patients (88.9%) had TERT promoter mutation at hotspot C228T (chr5: 1,295,228C>T), seven patients (9.7%) had the C250T (chr5: 1,295,250C>T) mutation, and one patient (1.4%) had the C228A (chr5: 1,295,228C>A) mutation. Clinicopathological characteristics were not significantly different between C228T and C250T mutations (Table 5).
RESULTS
- This study reviewed the prospectively collected data from 2,092 consecutive patients with thyroid carcinoma for the last two years in a real-world setting. Thus, we demonstrated the real-world situation of TERT promoter mutations in a large number of patients. The frequency of TERT promoter mutations was 3.4% in all types of thyroid carcinoma and 2.8% in PTC. In addition, the frequency of TERT promoter mutations was only 0.5% in PTMC but it was 5.8% in PTC with primary tumor size larger than 1 cm. Overall, TERT promoter mutational status was significantly associated with old age, male sex, large tumor size, advanced histological type, advanced T and N stage, and presence of distant metastasis.
- In Korea, the incidence of thyroid carcinoma abruptly increased after the introduction of high-resolution ultrasonography and peaked in 2012, and then decreased [18]. Since the introduction of the Revised Korean Thyroid Association management guidelines, most thyroid tumors of 1 cm or less do not undergo cytologic examination, and active surveillance is selected as an optional method of treatment [19]. However, if the tumor grows or progresses during observation, or if the patient strongly desires surgery, surgery is performed [20-22]. In Korea, approximately half of thyroid carcinoma patients undergo surgery for small tumors of less than 1 cm in diameter despite the effort to avoid overtreatment. As a consequence, more than half of the subjects in this study are diagnosed with PTMC (n=1,143). Therefore, we could provide real-world data for PTMC.
- In a meta-analysis, TERT promoter mutations were observed in 10% (4.5% to 25.5%) of patients with PTC, 17% (13.8% to 36.4%) of those with FTC, 40% (21.4% to 51.7%) of those with PDTC, and 40% (12.6% to 60.0%) of those with ATC [7-10,13]. de Biase et al. [23] reported the frequency of PTMC as 4.7%. Since, previous studies reported TERT promoter mutations in PTC were associated with clinicopathological features such as old age, and larger tumor size [10,11,23-26], we compare patients’ baseline characteristics between this study and previous studies (Supplemental Table S4). The mean age at diagnosis of wild-type TERT patients was similar to previous reports, and it was similar to or older than previous reports in patients with TERT promoter mutations. Also, the proportion of female patients in each group was similar.
- Despite the baseline characteristics being similar to previous reports, we found that the frequency of TERT promoter mutations is much lower in real-world data. The frequency is still lower than previous reports when analyzed in PTC with primary tumor size >1 cm. In addition, initial distant metastasis was not presented in any of the six patients with TERT promoter mutations in PTMC. The clinical significance of TERT promoter mutations might be lower when the primary tumor size is smaller, and this result is consistent with a previous report [23]. In PTMC, active surveillance is one of the treatment options [27]. Previous studies have tried to find biological markers to predict PTMC growth [28,29]. TERT promoter mutations are associated with poor prognosis; thus, Yabuta et al. [29] assessed 26 of 1,252 patients with molecular analysis during active surveillance. However, none of them had TERT promoter mutations. This result is understandable considering the low frequency of TERT promoter mutations in real-world data. The clinical significance of TERT promoter mutations might be lower when the primary tumor size is smaller, and this result is consistent with a previous report [23].
- TERT promoter mutations are rarely found in childhood thyroid carcinoma, whereas they are detected more commonly in the elderly [7,9,30-32]. During proliferation in the cells of older individuals, telomere dysfunction or further telomere crisis occurs because of shorter telomeres and deficient telomerase. This result triggers genomic instability and induces the development of TERT promoter mutations [26]. In the present study, the frequency of TERT promoter mutations increased significantly with age (OR, 1.13; P<0.001). Furthermore, the significance was present consistently in categorical analysis (P for trend <0.001). This result was more predominant in women. No female patient aged younger than 29 years had TERT promoter mutations, 0.3% of the females aged between 30 and 39 years had mutations, and 0.9% in those aged between 40 and 49 years, whereas the frequency of TERT promoter mutations was up to 3.0% in male patients aged under 49 years. Although some studies have provided different results, the majority of previous studies have reported that TERT promoter mutations were found more frequently in men than in women [33]. In addition, the frequency of TERT promoter mutations increased significantly as the tumor size increased (OR, 2.02; P<0.001). In patients categorized according to primary tumor size, ORs were significantly increased as the primary tumor size increased. This result is consistent with previous reports showing that the frequency of TERT promoter mutations was higher in large tumors [7,9].
- Two mutations in the TERT promoter (chr5: 1295228C>T, termed C228T, and chr5: 1295250C>T, termed C250T) were found in follicular cell-derived thyroid carcinoma [8,10,26,34-36]. C228T was reported to be far more dominant than C250T, and these two mutations occur in a mutually exclusive manner. Their mutual exclusivity suggests that each of them may play a specific role in thyroid tumorigenesis [8,9,37]. In this study, C228T mutations were found more frequently than C250T mutations, which is consistent with a previous report. One patient with tall cell variant PTC had C228A mutations. There were no significant differences in clinicopathological characteristics between C228T and C250T. However, these results need to be validated in larger studies because the number of C250T patients was too small.
- TERT promoter mutations have been reported to be highly prevalent in tumors with aggressive or dedifferentiated histology [7-9]. In this study, similar results were found. The frequencies of TERT promoter mutations were 18.4% (7 of 38) in FTC, 7.1% (1 of 14) in HTC, 23.0% (3 of 13) in PDTC, and 57.1% (4 of 7) in ATC, whereas the frequency was 2.8% (57 of 2020) in PTC. In PTC, TERT promoter mutations were found more frequently in the tall cell variants than in classic or follicular variants (7.6% vs. 2.5% vs. 2.4%), which was consistent with previous reports. TERT promoter mutations have been reported to be more prevalent in the tall cell variants than classic or follicular variants [8,9,38]. On the other hand, the frequency of TERT promoter mutations in HTC was lower than that in previous reports [34,39]. Chindris et al. [39] assayed TERT promoter sequence variation in 61 of 173 patients with HTC treated at Mayo Clinic over 11 years. The authors reported that the frequency was 13.1% (widely invasive 6/48 vs. minimally invasive 2/13) [39]. Landa et al. [34] reported that the frequency in HTC was 16.0%, but TERT promoter mutations were restricted to widely invasive HTC and did not occur in minimally invasive HTC (widely invasive 4/17 vs. minimally invasive 0/8). The incidence of HTC in Korea is very low and accounts for less than 1% of all thyroid carcinomas. In this study, the incidence of HTC was only 0.7% of all thyroid carcinomas, and only 14 patients with HTC were included. Therefore, it is difficult to compare the results of this study with other results because of the large differences in subject numbers. Nevertheless, one of the 14 (7.1%) HTC patients had TERT promoter mutations, and the histological subtype was encapsulated angioinvasive type. According to a previous study, a high expression level of TERT was seen in two structural rearrangements in widely invasive FTC [40]. Thus, high TERT alteration frequency can have TERT mutations such as fusion as well as TERT promoter mutations. Since we performed targeted sequencing methods that could not detected structural rearrangement, there might be more tumors with TERT rearrangements.
- Previous reports showed that the TERT promoter mutations are highly prevalent in advanced stages and distant metastasis [9-11,13,33,34,37], and the results of this study were consistent with this finding. In addition, the frequency of TERT promoter mutations was significantly higher in men than in women (OR, 2.05; P=0.003). Although some studies have obtained different results, the majority of previous studies have reported that TERT promoter mutations are found more frequently in men than in women [33].
- Given the low mortality rate despite the increased incidence of thyroid carcinoma, aggressive treatment is necessary only for a small number of patients with thyroid carcinoma, and therefore it is very important to find a prognostic factor to discriminate these patients in advance. Among the many proposed prognostic factors, TERT promoter mutations are reported to be a powerful marker of poor prognosis, independent of tumor histological type [41]. However, previous studies on TERT promoter mutations were retrospectively conducted on a limited number of subjects. In the present study, we prospectively tested TERT promoter mutations in a large number of patients with thyroid carcinoma. Therefore, this study is the first attempt to investigate the real-world frequency of TERT promoter mutations in thyroid carcinoma patients. The real-world frequency of TERT promoter mutations seems lower than expected. In particular, the frequency of TERT promoter mutations in PTMC, young age, and female patients was very low. However, we could not obtain long-term outcomes because of the short follow-up duration. Thus, further studies would be needed to provide long-term outcomes.
- In conclusion, the frequency of TERT promoter mutations was 3.4% in all types of thyroid carcinoma, and it was 2.8% in PTC. However, the frequency of TERT promoter mutations was only 0.5% in PTMC. The frequency of TERT promoter mutations was significantly higher in old age, large tumors, and aggressive histology. There were no clinicopathological differences between C228T and C250T. This study provides basic data for further investigations on TERT promoter mutations.
DISCUSSION
-
Acknowledgements
- This research has been presented as poster presentation at the 2022 Korean Endocrine Society Annual Congress, which was held in Seoul, Korea 7th to 9th April, 2022. The poster was awarded a prize during the congress.
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTION
Conception or design: J.H.C.
Acquisition, analysis, or interpretation of data: H.Y., H.P., H.J.R., J.H., J.S.K., Y.L.O., J.H.C., J.H.K., J.S.K., H.W.J., T.H.K., S.W.K.
Drafting the work or revising: H.Y., H.P.
Final approval of the manuscript: J.H.C.
Article information
Supplementary Information
Supplemental Table S1.
Supplemental Table S2.
Supplemental Table S3.
Supplemental Table S4.
Supplemental Fig. S1.
Supplemental Fig. S2.

| Clinical characteristic | Mutation-type (n=72) | Wild-type (n=2,020) | Odds ratio (95% CI) | P value |
|---|---|---|---|---|
| Age, yr | 62.5±12.9 | 45.0±12.6 | 1.12 (1.09–1.14) | <0.001 |
| <55 | 17 (23.6) | 1,541 (76.3) | 1.00 (reference) | |
| ≥55 | 55 (76.4) | 479 (23.7) | 10.41 (5.98–18.10) | <0.001 |
| Age, yra | ||||
| 10–19 | 0 | 19 (0.9) | 1.00 (reference) | |
| 20–29 | 1 (1.4) | 203 (10.0) | Non-estimable | |
| 30–39 | 3 (4.2) | 499 (24.7) | Non-estimable | |
| 40–49 | 7 (9.7) | 578 (28.6) | Non-estimable | |
| 50–59 | 15 (20.8) | 437 (21.6) | Non-estimable | |
| 60–69 | 23 (31.9) | 228 (11.3) | Non-estimable | |
| 70–79 | 18 (25.0) | 53 (2.6) | Non-estimable | |
| ≥80 | 5 (6.9) | 3 (0.1) | Non-estimable | |
| Sex | ||||
| Female | 42 (58.3) | 1,497 (74.1) | 1.00 (reference) | |
| Male | 30 (41.7) | 523 (25.9) | 2.05 (1.27–3.30) | 0.003 |
| Tumor size, cm | 3.20±1.95 | 1.27±1.04 | 2.02 (1.78–2.29) | <0.001 |
| 0.1–1.0 | 6 (8.3) | 1,138 (56.3) | 1.00 (reference) | |
| 1.1–2.0 | 21 (29.2) | 586 (29.0) | 6.78 (2.73–16.93) | <0.001 |
| 2.1–3.0 | 14 (19.4) | 161 (8.0) | 16.49 (6.25–43.53) | <0.001 |
| 3.1–4.0 | 10 (13.9) | 73 (3.6) | 25.98 (9.19–73.47) | <0.001 |
| 4.1–5.0 | 7 (9.7) | 31 (1.5) | 42.93 (13.60–134.90) | <0.001 |
| 5.1–8.5 | 14 (19.4) | 32 (1.5) | 85.66 (30.86–237.72) | <0.001 |
| Histological type | ||||
| Papillary thyroid carcinoma | 57 (79.2) | 1,963 (97.2) | 1.00 (reference) | |
| Follicular thyroid carcinoma | 7 (9.7) | 31 (1.5) | 7.78 (3.29–18.40) | <0.001 |
| Hurthle cell thyroid carcinoma | 1 (1.4) | 13 (0.6) | 2.65 (0.34–20.60) | 0.352 |
| Poorly differentiated thyroid carcinoma | 3 (4.2) | 10 (0.5) | 10.33 (2.77–38.55) | 0.001 |
| Anaplastic thyroid carcinoma | 4 (5.6) | 3 (0.1) | 45.92 (10.04–209.93) | <0.001 |
| Pathologic T category | ||||
| T1 | 19 (26.4) | 1,652 (81.8) | 1.00 (reference) | |
| T2 | 6 (8.3) | 198 (9.8) | 2.64 (1.04–6.68) | 0.041 |
| T3 | 20 (27.8) | 155 (7.7) | 11.22 (5.86–21.47) | <0.001 |
| T4 | 27 (37.5) | 15 (0.7) | 156.51 (72.00–340.20) | <0.001 |
| Pathologic N categoryb | ||||
| Nx | 13 (18.1) | 347 (17.2) | - | |
| N0 | 21 (29.2) | 750 (37.1) | 1.00 (reference) | |
| N1a | 15 (20.8) | 654 (32.4) | 0.82 (0.42–1.60) | 0.560 |
| N1b | 23 (31.9) | 269 (13.3) | 3.05 (1.66–5.61) | <0.001 |
| Initial distant metastasis | ||||
| Absent | 60 (83.3) | 2,000 (99.0) | 1.00 (reference) | |
| Present | 12 (16.7) | 20 (1.0) | 20.0 (9.35–42.78) | <0.001 |
| Clinical characteristic |
PTC ≤1 cm (n=1,143) |
PTC >1 cm (n=877) |
||||
|---|---|---|---|---|---|---|
| Mutation-type (n=6) | Wild-type (n=1,137) | P value | Mutation-type (n=51) | Wild-type (n=826) | P value | |
| Age, yr | 60.5±15.6 | 45.5±11.6 | 0.021 | 63.7±11.2 | 44.0±13.5 | <0.001 |
| <55 | 3 (50.0) | 877 (77.1) | 0.139 | 9 (17.6) | 631 (76.4) | <0.001 |
| ≥55 | 3 (50.0) | 260 (22.9) | 42 (82.4) | 195 (23.6) | ||
| Sex | ||||||
| Female | 4 (66.7) | 857 (75.4) | 0.640 | 28 (54.9) | 595 (72.0) | 0.009 |
| Male | 2 (33.3) | 280 (24.6) | 23 (45.1) | 231 (28.0) | ||
| Pathologic T category | ||||||
| T1 | 5 (83.3) | 1,110 (97.6) | 0.027 | 11 (21.6) | 527 (63.8) | <0.001 |
| T2 | 0 | 1 (0.1) | 5 (9.8) | 173 (20.9) | ||
| T3 | 0 | 24 (2.1) | 14 (27.5) | 113 (13.7) | ||
| T4 | 1 (16.7) | 2 (0.2) | 21 (41.2) | 13 (1.6) | ||
| Pathologic N categorya | ||||||
| Nx | 2 (33.3) | 177 (15.6) | 0.043 | 5 (9.8) | 138 (16.7) | 0.037 |
| N0 | 1 (16.7) | 510 (44.9) | 14 (27.5) | 222 (26.9) | ||
| N1a | 1 (16.7) | 365 (32.1) | 12 (23.5) | 283 (34.3) | ||
| N1b | 2 (33.3) | 85 (7.5) | 20 (39.2) | 183 (22.2) | ||
| Initial distant metastasis | ||||||
| Absent | 6 (100.0) | 1,133 (99.6) | >0.999 | 46 (90.2) | 814 (98.5) | 0.002 |
| Present | 0 | 4 (0.4) | 5 (9.8) | 12 (1.5) | ||
| TERT promoter mutation | ||||||
| C228T mutation | 5 (83.3) | - | 45 (88.2) | - | ||
| C250T mutation | 1 (16.7) | - | 5 (9.8) | - | ||
| C228A mutation | 0 | - | 1 (2.0) | - | ||
| Clinical characteristic |
Age <55 years (n=1,520) |
Age ≥55 years (n=500) |
||||
|---|---|---|---|---|---|---|
| Mutation-type (n=12) | Wild-type (n=1,508) | P value | Mutation-type (n=45) | Wild-type (n=455) | P value | |
| Age, yr | 46.8±5.9 | 39.7±8.7 | 0.005 | 67.8±8.3 | 62.0±5.7 | <0.001 |
| Sex | ||||||
| Female | 5 (41.7) | 1,115 (73.9) | 0.019 | 27 (60.0) | 337 (74.1) | 0.043 |
| Male | 7 (58.3) | 393 (26.1) | 18 (40.0) | 118 (25.9) | ||
| Tumor size, cm | 1.57±1.17 | 1.22±0.97 | 0.202 | 3.17±1.68 | 1.17±0.91 | <0.001 |
| 0.1–1.0 | 3 (25.0) | 877 (58.2) | 0.060 | 3 (6.7) | 260 (57.1) | <0.001 |
| 1.1–2.0 | 7 (58.3) | 428 (28.4) | 12 (26.7) | 148 (32.5) | ||
| 2.1–3.0 | 1 (8.3) | 118 (7.8) | 10 (22.2) | 27 (5.9) | ||
| 3.1–4.0 | 0 | 47 (3.1) | 9 (20.0) | 13 (2.9) | ||
| 4.1–5.0 | 1 (8.3) | 21 (1.4) | 3 (6.7) | 1 (0.2) | ||
| 5.1–8.5 | 0 | 17 (1.1) | 8 (17.8) | 6 (1.3) | ||
| Pathologic T category | ||||||
| T1 | 6 (50.0) | 1,246 (82.6) | <0.001 | 10 (22.2) | 391 (85.9) | <0.001 |
| T2 | 1 (8.3) | 139 (9.2) | 4 (8.9) | 35 (7.7) | ||
| T3 | 3 (25.0) | 111 (7.4) | 11 (24.4) | 26 (5.7) | ||
| T4 | 2 (16.7) | 12 (0.8) | 20 (44.4) | 3 (0.7) | ||
| Pathologic N categorya | ||||||
| Nx | 3 (25.0) | 223 (14.8) | >0.999 | 4 (8.9) | 92 (20.2) | <0.001 |
| N0 | 4 (33.3) | 536 (35.5) | 11 (24.4) | 196 (43.1) | ||
| N1a | 4 (33.3) | 530 (35.1) | 9 (20.0) | 118 (25.9) | ||
| N1b | 1 (8.3) | 219 (14.5) | 21 (46.7) | 49 (10.8) | ||
| Initial distant metastasis | ||||||
| Absent | 12 (100.0) | 1,494 (99.1) | >0.999 | 40 (88.9) | 453 (99.6) | <0.001 |
| Present | 0 | 14 (0.9) | 5 (11.1) | 2 (0.4) | ||
| TERT promoter mutation | ||||||
| C228T mutation | 10 (83.3) | - | 40 (88.9) | - | ||
| C250T mutation | 2 (16.7) | - | 4 (8.9) | - | ||
| C228A mutation | 0 | - | 1 (2.2) | - | ||
| Clinical characteristic | C228T (n=64) | C250T (n=7) | P value |
|---|---|---|---|
| Age, yr | 63.0±13.1 | 56.7±10.3 | 0.222 |
| <55 | 14 (21.9) | 3 (42.9) | 0.346 |
| ≥55 | 50 (78.1) | 4 (57.1) | |
| Sex | |||
| Female | 37 (57.8) | 4 (57.1) | >0.999 |
| Male | 27 (42.2) | 3 (42.9) | |
| Tumor size, cm | 3.3±2.0 | 2.6±1.4 | 0.363 |
| Pathologic T category | |||
| T1 | 18 (28.1) | 1 (14.3) | 0.796 |
| T2 | 5 (7.8) | 1 (14.3) | |
| T3 | 18 (28.1) | 2 (28.6) | |
| T4 | 23 (35.9) | 3 (42.9) | |
| Pathologic N categorya | |||
| Nx | 11 (17.2) | 2 (28.6) | >0.999 |
| N0 | 18 (28.1) | 2 (28.6) | |
| N1a | 14 (21.9) | 1 (14.3) | |
| N1b | 21 (32.8) | 2 (28.6) | |
| Initial distant metastasis | |||
| Absent | 52 (81.3) | 7 (100.0) | 0.593 |
| Present | 12 (18.8) | 0 | |
| Histological type | |||
| Papillary thyroid carcinoma | 50 (78.1) | 6 (85.7) | 0.477 |
| Follicular thyroid carcinoma | 7 (10.9) | 0 | |
| Hurthle cell thyroid carcinoma | 1 (1.6) | 0 | |
| Poorly differentiated thyroid carcinoma | 2 (3.1) | 1 (14.3) | |
| Anaplastic thyroid carcinoma | 4 (6.3) | 0 |
- 1. La Vecchia C, Malvezzi M, Bosetti C, Garavello W, Bertuccio P, Levi F, et al. Thyroid cancer mortality and incidence: a global overview. Int J Cancer 2015;136:2187–95.ArticlePubMed
- 2. Davies L, Morris LG, Haymart M, Chen AY, Goldenberg D, Morris J, et al. American Association of Clinical Endocrinologists and American College of Endocrinology Disease state clinical review: the increasing incidence of thyroid cancer. Endocr Pract 2015;21:686–96.ArticlePubMedPMC
- 3. Li M, Brito JP, Vaccarella S. Long-term declines of thyroid cancer mortality: an international age-period-cohort analysis. Thyroid 2020;30:838–46.ArticlePubMed
- 4. DeGroot LJ, Kaplan EL, McCormick M, Straus FH. Natural history, treatment, and course of papillary thyroid carcinoma. J Clin Endocrinol Metab 1990;71:414–24.ArticlePubMed
- 5. Hay ID, Bergstralh EJ, Goellner JR, Ebersold JR, Grant CS. Predicting outcome in papillary thyroid carcinoma: development of a reliable prognostic scoring system in a cohort of 1779 patients surgically treated at one institution during 1940 through 1989. Surgery 1993;114:1050–7.PubMed
- 6. Mazzaferri EL, Kloos RT. Clinical review 128: current approaches to primary therapy for papillary and follicular thyroid cancer. J Clin Endocrinol Metab 2001;86:1447–63.PubMed
- 7. Kim TH, Kim YE, Ahn S, Kim JY, Ki CS, Oh YL, et al. TERT promoter mutations and long-term survival in patients with thyroid cancer. Endocr Relat Cancer 2016;23:813–23.ArticlePubMed
- 8. Liu X, Bishop J, Shan Y, Pai S, Liu D, Murugan AK, et al. Highly prevalent TERT promoter mutations in aggressive thyroid cancers. Endocr Relat Cancer 2013;20:603–10.ArticlePubMedPMC
- 9. Alzahrani AS, Alsaadi R, Murugan AK, Sadiq BB. TERT promoter mutations in thyroid cancer. Horm Cancer 2016;7:165–77.ArticlePubMedPMCPDF
- 10. Melo M, da Rocha AG, Vinagre J, Batista R, Peixoto J, Tavares C, et al. TERT promoter mutations are a major indicator of poor outcome in differentiated thyroid carcinomas. J Clin Endocrinol Metab 2014;99:E754–65.ArticlePubMedPMC
- 11. Xing M, Liu R, Liu X, Murugan AK, Zhu G, Zeiger MA, et al. BRAF V600E and TERT promoter mutations cooperatively identify the most aggressive papillary thyroid cancer with highest recurrence. J Clin Oncol 2014;32:2718–26.ArticlePubMedPMC
- 12. George JR, Henderson YC, Williams MD, Roberts DB, Hei H, Lai SY, et al. Association of TERT promoter mutation, but not BRAF mutation, with increased mortality in PTC. J Clin Endocrinol Metab 2015;100:E1550–9.ArticlePubMedPMC
- 13. Gandolfi G, Ragazzi M, Frasoldati A, Piana S, Ciarrocchi A, Sancisi V. TERT promoter mutations are associated with distant metastases in papillary thyroid carcinoma. Eur J Endocrinol 2015;172:403–13.ArticlePubMed
- 14. Bullock M, Ren Y, O’Neill C, Gill A, Aniss A, Sywak M, et al. TERT promoter mutations are a major indicator of recurrence and death due to papillary thyroid carcinomas. Clin Endocrinol (Oxf) 2016;85:283–90.PubMedPMC
- 15. Park J, Lee S, Kim K, Park H, Ki CS, Oh YL, et al. TERT promoter mutations and the 8th edition TNM classification in predicting the survival of thyroid cancer patients. Cancers (Basel) 2021;13:648.ArticlePubMedPMC
- 16. Park J, Lee S, Park J, Park H, Ki CS, Oh YL, et al. Proposal of a new prognostic model for differentiated thyroid cancer with TERT promoter mutations. Cancers (Basel) 2021;13:2943.ArticlePubMedPMC
- 17. Park H, Shin HC, Yang H, Heo J, Ki CS, Kim HS, et al. Molecular classification of follicular thyroid carcinoma based on TERT promoter mutations. Mod Pathol 2022;35:186–92.ArticlePubMedPMCPDF
- 18. Oh CM, Lim J, Jung YS, Kim Y, Jung KW, Hong S, et al. Decreasing trends in thyroid cancer incidence in South Korea: what happened in South Korea? Cancer Med 2021;10:4087–96.ArticlePubMedPMCPDF
- 19. Yi KH, Lee EK, Kang HC, Koh Y, Kim SW, Kim IJ, et al. 2016 Revised Korean Thyroid Association management guidelines for patients with thyroid nodules and thyroid cancer. Int J Thyroidol 2016;9:59–126.ArticlePDF
- 20. Kim HI, Jang HW, Ahn HS, Ahn S, Park SY, Oh YL, et al. High serum TSH level is associated with progression of papillary thyroid microcarcinoma during active surveillance. J Clin Endocrinol Metab 2018;103:446–51.ArticlePubMedPDF
- 21. Oh HS, Ha J, Kim HI, Kim TH, Kim WG, Lim DJ, et al. Active surveillance of low-risk papillary thyroid microcarcinoma: a multi-center cohort study in Korea. Thyroid 2018;28:1587–94.ArticlePubMed
- 22. Jin M, Kim HI, Ha J, Jeon MJ, Kim WG, Lim DJ, et al. Tumor volume doubling time in active surveillance of papillary thyroid microcarcinoma: a multicenter cohort study in Korea. Thyroid 2021;31:1494–501.ArticlePubMed
- 23. de Biase D, Gandolfi G, Ragazzi M, Eszlinger M, Sancisi V, Gugnoni M, et al. TERT promoter mutations in papillary thyroid microcarcinomas. Thyroid 2015;25:1013–9.ArticlePubMed
- 24. Muzza M, Colombo C, Rossi S, Tosi D, Cirello V, Perrino M, et al. Telomerase in differentiated thyroid cancer: promoter mutations, expression and localization. Mol Cell Endocrinol 2015;399:288–95.ArticlePubMed
- 25. Liu X, Qu S, Liu R, Sheng C, Shi X, Zhu G, et al. TERT promoter mutations and their association with BRAF V600E mutation and aggressive clinicopathological characteristics of thyroid cancer. J Clin Endocrinol Metab 2014;99:E1130–6.ArticlePubMedPMC
- 26. Liu T, Wang N, Cao J, Sofiadis A, Dinets A, Zedenius J, et al. The age- and shorter telomere-dependent TERT promoter mutation in follicular thyroid cell-derived carcinomas. Oncogene 2014;33:4978–84.ArticlePubMedPDF
- 27. Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016;26:1–133.ArticlePubMedPMC
- 28. Hirokawa M, Kudo T, Ota H, Suzuki A, Miyauchi A. Pathological characteristics of low-risk papillary thyroid microcarcinoma with progression during active surveillance. Endocr J 2016;63:805–10.ArticlePubMed
- 29. Yabuta T, Matsuse M, Hirokawa M, Yamashita S, Mitsutake N, Miyauchi A. TERT promoter mutations were not found in papillary thyroid microcarcinomas that showed disease progression on active surveillance. Thyroid 2017;27:1206–7.ArticlePubMed
- 30. Ballester LY, Sarabia SF, Sayeed H, Patel N, Baalwa J, Athanassaki I, et al. Integrating molecular testing in the diagnosis and management of children with thyroid lesions. Pediatr Dev Pathol 2016;19:94–100.ArticlePubMedPDF
- 31. Onder S, Ozturk Sari S, Yegen G, Sormaz IC, Yilmaz I, Poyrazoglu S, et al. Classic architecture with multicentricity and local recurrence, and absence of TERT promoter mutations are correlates of BRAF (V600E) harboring pediatric papillary thyroid carcinomas. Endocr Pathol 2016;27:153–61.ArticlePubMedPDF
- 32. Oishi N, Kondo T, Nakazawa T, Mochizuki K, Inoue T, Kasai K, et al. Frequent BRAF V600E and absence of TERT promoter mutations characterize sporadic pediatric papillary thyroid carcinomas in Japan. Endocr Pathol 2017;28:103–11.ArticlePubMedPDF
- 33. Yang J, Gong Y, Yan S, Chen H, Qin S, Gong R. Association between TERT promoter mutations and clinical behaviors in differentiated thyroid carcinoma: a systematic review and meta-analysis. Endocrine 2020;67:44–57.ArticlePubMedPMCPDF
- 34. Landa I, Ganly I, Chan TA, Mitsutake N, Matsuse M, Ibrahimpasic T, et al. Frequent somatic TERT promoter mutations in thyroid cancer: higher prevalence in advanced forms of the disease. J Clin Endocrinol Metab 2013;98:E1562–6.ArticlePubMedPMCPDF
- 35. Huang FW, Hodis E, Xu MJ, Kryukov GV, Chin L, Garraway LA. Highly recurrent TERT promoter mutations in human melanoma. Science 2013;339:957–9.ArticlePubMedPMC
- 36. Vinagre J, Almeida A, Populo H, Batista R, Lyra J, Pinto V, et al. Frequency of TERT promoter mutations in human cancers. Nat Commun 2013;4:2185.ArticlePubMedPDF
- 37. Liu R, Xing M. TERT promoter mutations in thyroid cancer. Endocr Relat Cancer 2016;23:R143–55.ArticlePubMedPMC
- 38. Qasem E, Murugan AK, Al-Hindi H, Xing M, Almohanna M, Alswailem M, et al. TERT promoter mutations in thyroid cancer: a report from a Middle Eastern population. Endocr Relat Cancer 2015;22:901–8.ArticlePubMed
- 39. Chindris AM, Casler JD, Bernet VJ, Rivera M, Thomas C, Kachergus JM, et al. Clinical and molecular features of Hürthle cell carcinoma of the thyroid. J Clin Endocrinol Metab 2015;100:55–62.ArticlePubMedPDF
- 40. Yoo SK, Song YS, Lee EK, Hwang J, Kim HH, Jung G, et al. Integrative analysis of genomic and transcriptomic characteristics associated with progression of aggressive thyroid cancer. Nat Commun 2019;10:2764.ArticlePubMedPMCPDF
- 41. Liu R, Bishop J, Zhu G, Zhang T, Ladenson PW, Xing M. Mortality risk stratification by combining BRAF V600E and TERT promoter mutations in papillary thyroid cancer: genetic duet of BRAF and TERT promoter mutations in thyroid cancer mortality. JAMA Oncol 2017;3:202–8.ArticlePubMed
References
Figure & Data
References
Citations
-
TERT Promoter Mutations Frequency Across Race, Sex, and Cancer Type
Talal El Zarif, Marc Machaalani, Rashad Nawfal, Amin H Nassar, Wanling Xie, Toni K Choueiri, Mark Pomerantz
The Oncologist.2024; 29(1): 8. CrossRef - Gene mutations as predictors of central lymph mode metastasis in cN0 PTC: A meta‐analysis
Jiaqi Ji, Xinlong Shi
Clinical Genetics.2024; 105(2): 130. CrossRef - Risk stratification by combining common genetic mutations and TERT promoter methylation in papillary thyroid cancer
Ye Sang, Guanghui Hu, Junyu Xue, Mengke Chen, Shubin Hong, Rengyun Liu
Endocrine.2024;[Epub] CrossRef - Shortened telomere length in peripheral blood leukocytes is associated with cumulative radioactive iodine doses in patients with differentiated thyroid carcinoma
Hoonsung Choi, Sun Wook Cho, Hwan Hee Kim, Ka Hee Yi, Do Joon Park, Young Joo Park
Cancer.2024;[Epub] CrossRef - Deciphering the Functions of Telomerase Reverse Transcriptase in Head and Neck Cancer
Tsung-Jang Yeh, Chi-Wen Luo, Jeng-Shiun Du, Chien-Tzu Huang, Min-Hung Wang, Tzer-Ming Chuang, Yuh-Ching Gau, Shih-Feng Cho, Yi-Chang Liu, Hui-Hua Hsiao, Li-Tzong Chen, Mei-Ren Pan, Hui-Ching Wang, Sin-Hua Moi
Biomedicines.2023; 11(3): 691. CrossRef - 2023 Korean Thyroid Association Management Guidelines for Patients with Thyroid Nodules
Young Joo Park, Eun Kyung Lee, Young Shin Song, Soo Hwan Kang, Bon Seok Koo, Sun Wook Kim, Dong Gyu Na, Seung-Kuk Baek, So Won Oh, Min Kyoung Lee, Sang-Woo Lee, Young Ah Lee, Yong Sang Lee, Ji Ye Lee, Dong-Jun Lim, Leehi Joo, Yuh-Seog Jung, Chan Kwon Jung
International Journal of Thyroidology.2023; 16(1): 1. CrossRef - Thyroid Cancer, Iodine, and Gene Mutation
Jae Hoon Chung
International Journal of Thyroidology.2023; 16(1): 89. CrossRef - Mortality rate and causes of death in papillary thyroid microcarcinoma
Jung Heo, Hyun Jin Ryu, Hyunju Park, Tae Hyuk Kim, Sun Wook Kim, Young Lyun Oh, Jae Hoon Chung
Endocrine.2023; 83(3): 671. CrossRef - TERT promoter mutations in thyroid cancer
Michiko Matsuse, Norisato Mitsutake
Endocrine Journal.2023; 70(11): 1035. CrossRef - TERT Promoter and BRAF V600E Mutations in Papillary Thyroid Cancer: A Single-Institution Experience in Korea
Min Jhi Kim, Jin Kyong Kim, Gi Jeong Kim, Sang-Wook Kang, Jandee Lee, Jong Ju Jeong, Woong Youn Chung, Daham Kim, Kee-Hyun Nam
Cancers.2022; 14(19): 4928. CrossRef - Frequency of TERT Promoter Mutations in Real-World Analysis of 2,092 Thyroid Carcinoma Patients (Endocrinol Metab 2022;37:652-63, Heera Yang et al.)
Hyunju Park, Jae Hoon Chung
Endocrinology and Metabolism.2022; 37(6): 949. CrossRef - Frequency of TERT Promoter Mutations in Real-World Analysis of 2,092 Thyroid Carcinoma Patients (Endocrinol Metab 2022;37:652-63, Heera Yang et al.)
Sue Youn Kim, Chan Kwon Jung
Endocrinology and Metabolism.2022; 37(6): 947. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite