Effect of Cigarette Smoking on Thyroid Cancer: Meta-Analysis
Article information

Abstract
Background
Although smoking is generally carcinogenic, its effect on thyroid cancers is still subject to controversy. The purpose of this study was to summarize the role of smoking in relation to thyroid cancer occurrence.
Methods
We performed a meta-analysis of 24 eligible studies: 21 case-control studies and three prospective cohort studies. The summary odds ratio (OR) and 95% confidence interval (CI) of all studies were acquired based on random effect model. Further subgroup analyses were conducted according to gender, histological type of thyroid cancer, and smoking status of patients for the case-control studies.
Results
The summary effect size indicated a negative association of smoking for thyroid cancer (OR, 0.798; 95% CI, 0.681 to 0.935). From the subgroup analyses for the case-control studies, reduced risk of thyroid cancer was observed in both men (OR, 0.734; 95% CI, 0.553 to 0.974) and women (OR, 0.792; 95% CI, 0.700 to 0.897). The protective effect of smoking was observed in studies in which thyroid cancer was limited to differentiated thyroid cancers (DTCs) (OR, 0.798; 95% CI, 0.706 to 0.902).
Conclusion
Our results suggests that smoking may have a protective effect on thyroid cancer, especially on DTCs. Further studies with larger sample sizes should be conducted in elucidating the dose and time dependent effect of smoking on thyroid cancer with specific focus on the types of thyroid cancers.
INTRODUCTION
Thyroid cancer incidence has rapidly increased in the recent decades [1]. Many assume that such increase is caused by the improvement of diagnostic modalities or facilitated access to healthcare service [1], but there are counter-arguments claiming that some portion of the increase may be caused by potentially carcinogenic factors such as exposure to iodine or other behavioral factors [1,2].
In general, active cigarette smoking is one of the most well-known causes of cancer. It has been labelled as a carcinogenic factor for 12 cancers in a report published by the International Agency for Research on Cancer [3]. The evidence is equivocal; however, in the case of thyroid cancers; while some data support the carcinogenic effect of smoking on thyroid cancer [4], others demonstrate no significant effect of smoking on thyroid cancer [5,6] and some even support the decreased risk of thyroid cancer associated with cigarette smoking [7,8]. Because of the discordant results of many individual studies, a meta-analysis was necessary to synthesize the results and increase the statistical power.
The aim of this study was to investigate and summarize the role of smoking in relation to thyroid cancer occurrence. The population of individual studies consisted of thyroid cancer patients from hospital-based cohorts whereas non-cancer participant data were derived from either community or hospital-based cohorts. The intervention of interest was the participants’ status of smoking (ever/current/former smoker—depending on the studies). The case patients were smokers whereas the control were non-smokers. The outcome was the number of subjects that were diagnosis with thyroid cancer during the study period in each group. Both prospective cohort and case-control studies were included. We conducted further subgroup analyses in order to elucidate the source of heterogeneity.
METHODS
The institutional board (GCIRB2019-329) approved this study. The inclusion criteria included case-control or prospective cohort studies published in English extracted from search results on PubMed, Embase, and the Cochrane Library for studies that had investigated the effect of smoking on thyroid cancer occurrence and were published prior to November 13, 2019. The search was conducted by combining the medical subject heading term ‘thyroid neoplasm’ with the following keywords: (1) cigarette, (2) smoking, (3) tobacco, and (4) nicotine. Two researchers independently extracted and reviewed the abstracts or full text of the articles. Based on the title, abstract, and full text, the relevance of the identified studies was assessed through a hierarchical approach. Any disagreement between the two researchers during the selection process was resolved by discussion with a substantial inter-rater agreement (kappa statistic=0.81; 95% confidence interval [CI], 0.69 to 0.91). After searching titles in PubMed (n=366), Embase (n=279), and the Cochrane Library (n=15), an abstract review was performed for 177 studies, and a full-text review was performed for 36 articles, the process which is summarized in Fig. 1. Thirteen studies were not included in this analysis owing to the following exclusion criteria: report on overlapping cohorts (n=4) [9–12], missing data on the number of smokers (n=4) [13–16], missing comparison of different smoking status groups (n=3) [17–19], no presentation of novel data (n=2) [20,21]. After the exclusions, 23 studies were included in the analyses. The study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Supplemental Table S1) [22].
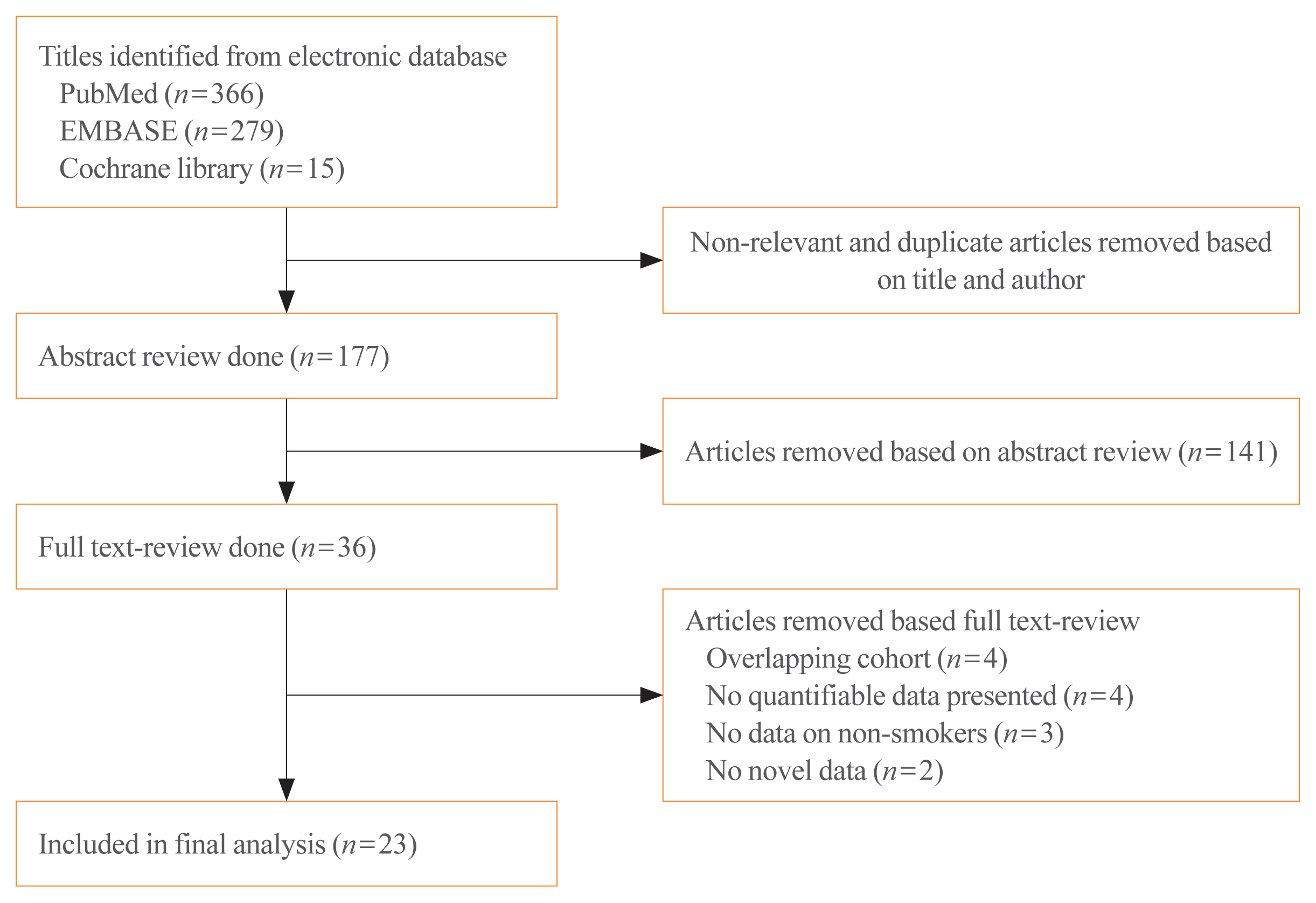
Study selection process.
Statistical analyses were conducted using the Comprehensive Meta-Analysis version 2.0 software (Biostat, Englewood, NJ, USA). The null hypothesis of no difference was rejected if P values were <0.05 or the 95% CI of risk estimates excluded 1. Because the individual studies consisted of a heterogeneous range of cigarette smoking assessment methods, random effects models [23] were used to calculate the odds ratios (OR) and 95% CIs based on analysis of Q-statistics. To estimate the degree of heterogeneity, P values for heterogeneity and I2 statistics were obtained, and a sensitivity analysis was subsequently performed to identify the source. In order to assess the risk of bias regarding our study, publication bias was visualized using a funnel plot and quantified with Egger’s linear regression by determining the asymmetry and was visualized using a funnel plot [24]. Furthermore, we assessed the quality of each individual studies using the Newcastle-Ottawa Scale which revealed a score of either 6 or 7 in all the studies [25].
To obtain the summary effect size, the data were grouped into cases (smokers) or controls (non-smokers). Because the definition of smoking status differed among the studies, it was necessary to redefine the case and control groups. Ever smokers (as presented in the individual studies) were defined as cases, and non-smokers (those who had never smoked) were defined as controls. Likewise, in articles that presented former and current smokers separately (as opposed to ever-smokers as a whole), subjects were combined to form the case group. Furthermore, the male and female groups were recognized as separate cohorts in studies where sex was analyzed separately.
The main analysis compared the effect size between the case and control groups of all studies in OR. Due to the heterogeneity of the studies, subsequent subgroup analyses were performed to retain homogeneity based on (1) the type of study (case-control vs. prospective cohort studies), (2) sex, and (3) the type of thyroid cancer (differentiated thyroid cancers [DTCs] vs. non-specified).
RESULTS
Twenty-three articles were selected for analyses, among which 21 [4,6,26–44] were case-control studies, and two were prospective cohorts (Table 1) [45,46]. In 15 studies [4,6,26,27,30,34–37,39–44] both sexes were analyzed; separate analyses for each sex were conducted in five studies [6,26,30,34,44]. Only women were analyzed in seven studies [28,29,31–33,45,46] and only men were studied in one [38]. Eleven studies analyzed the effect of smoking on DTCs specifically [6,29,31,34,36,38–40,44–46] and 13 assessed its effect on thyroid cancer without specifying the type [4,26–28,30,32,33,35,37,41–43,45,46].
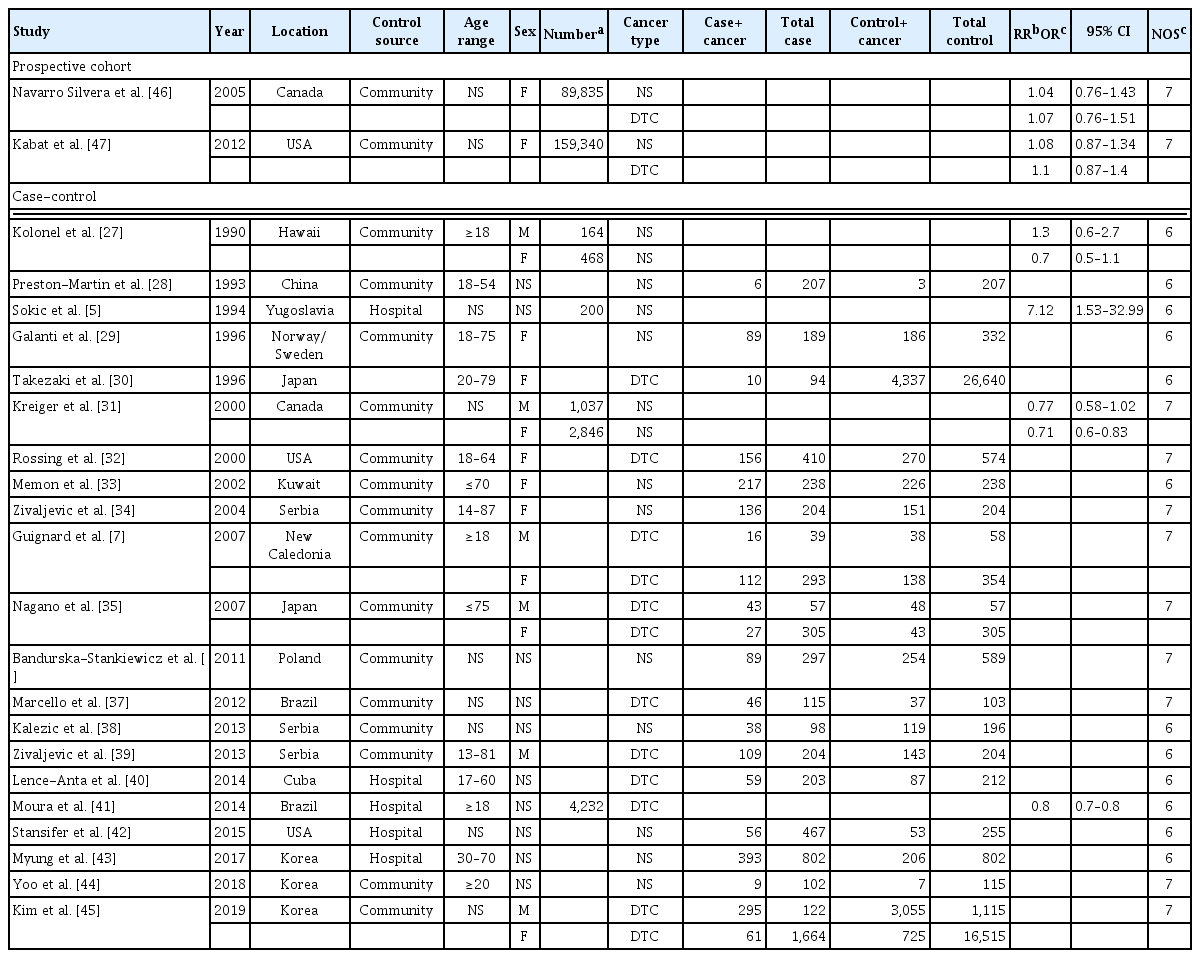
Baseline Characteristic of Studies Included in the Final Analysis
The summary effect size indicated the protective effect of smoking on thyroid cancer risk (OR, 0.798; 95% CI, 0.681 to 0.935; P value for heterogeneity >0.001; I2=84.89%) (Fig. 2). The funnel plot demonstrated symmetry, which was confirmed by an Egger’s intercept of −0.066 and a 2-tailed P value of 0.931 to address the issue of publication bias. Sensitivity analysis, performed by removing each study, demonstrated a consistent OR for all studies (Fig. 3).
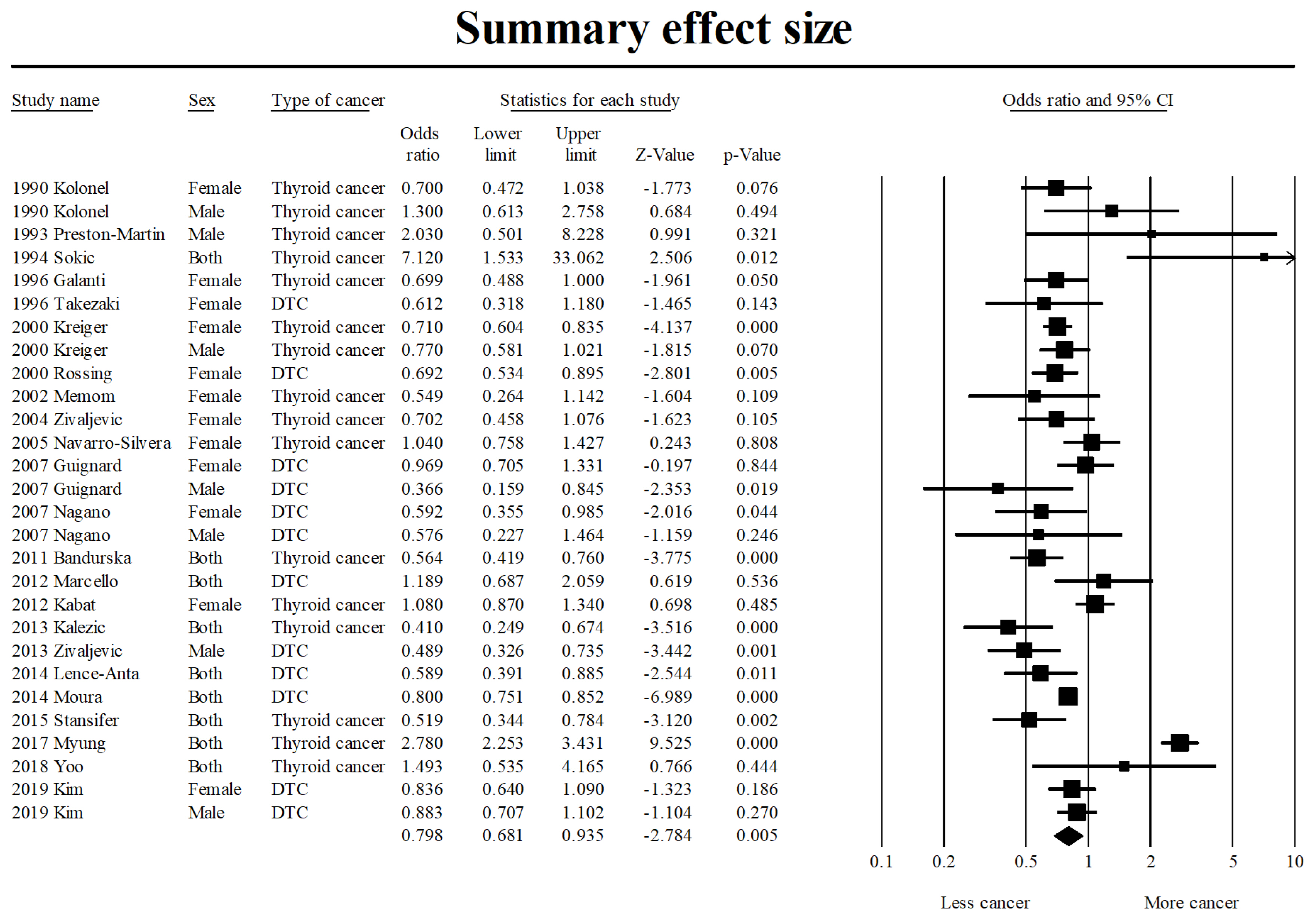
Summary effect size of association between smoking and thyroid cancer occurrence. DTC, differentiated thyroid cancer; CI, confidence interval.
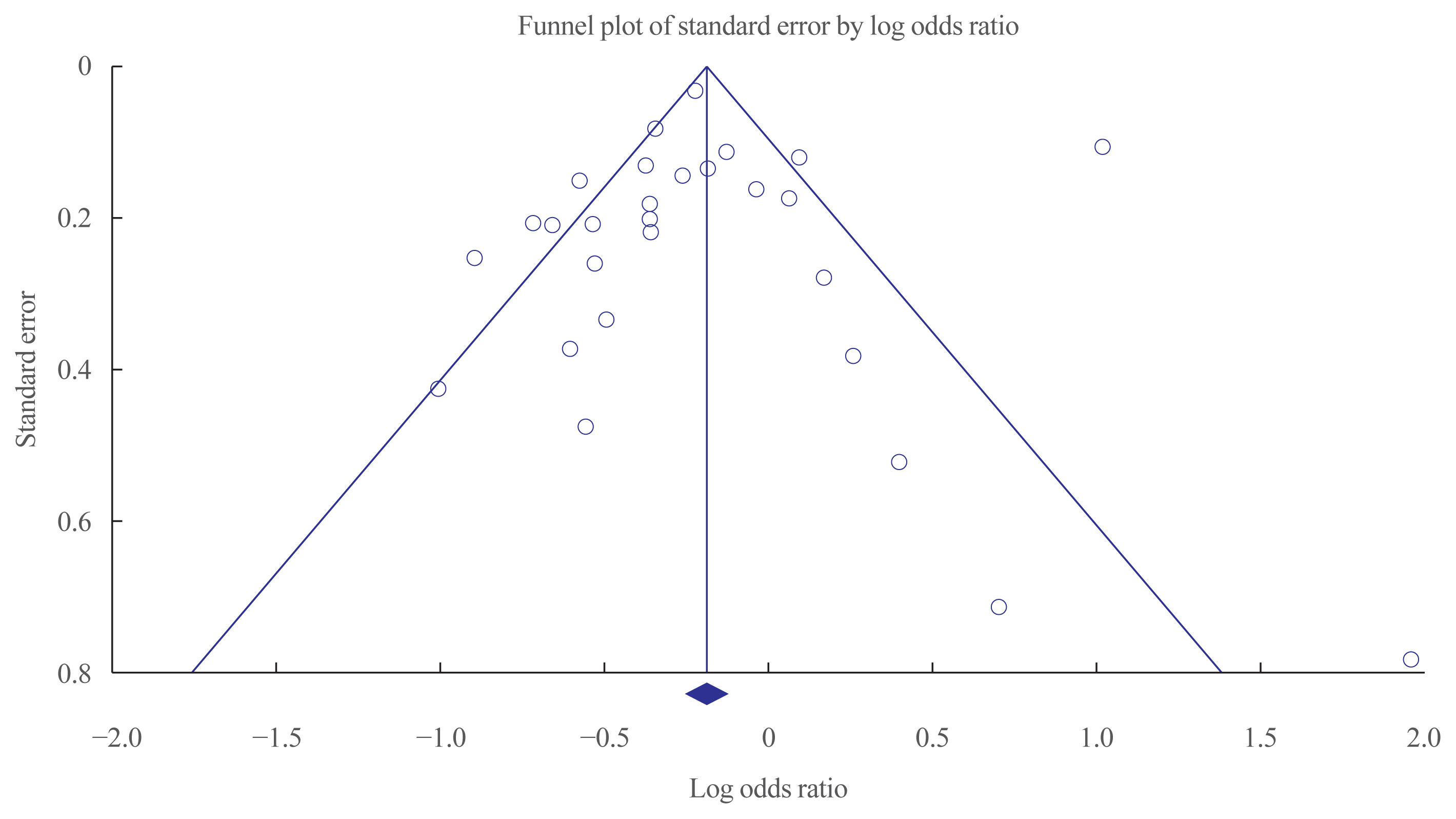
Funnel plot assessing publication bias.
In the subgroup analysis, the case control studies (OR, 0.779; 95% CI, 0.639 to 0.951) demonstrated the protective effect of smoking, but the two prospective cohorts (relative risk [RR], 1.090; 95 % CI, 0.897 to 1.326) did not. Furthermore, a reduced risk of thyroid cancer was observed both in male smokers (OR, 0.734; 95% CI, 0.553 to 0.974) and female smokers (OR, 0.792; 95% CI, 0.700 to 0.897). The observed protective effect was more pronounced in studies in which thyroid cancer was specified as DTC (OR, 0.798; 95% CI, 0.706 to 0.902) (Fig. 4), but such an effect was not observed for studies in which the type of thyroid cancer was not specified (OR, 0.896; 95% CI, 0.663 to 1.211).
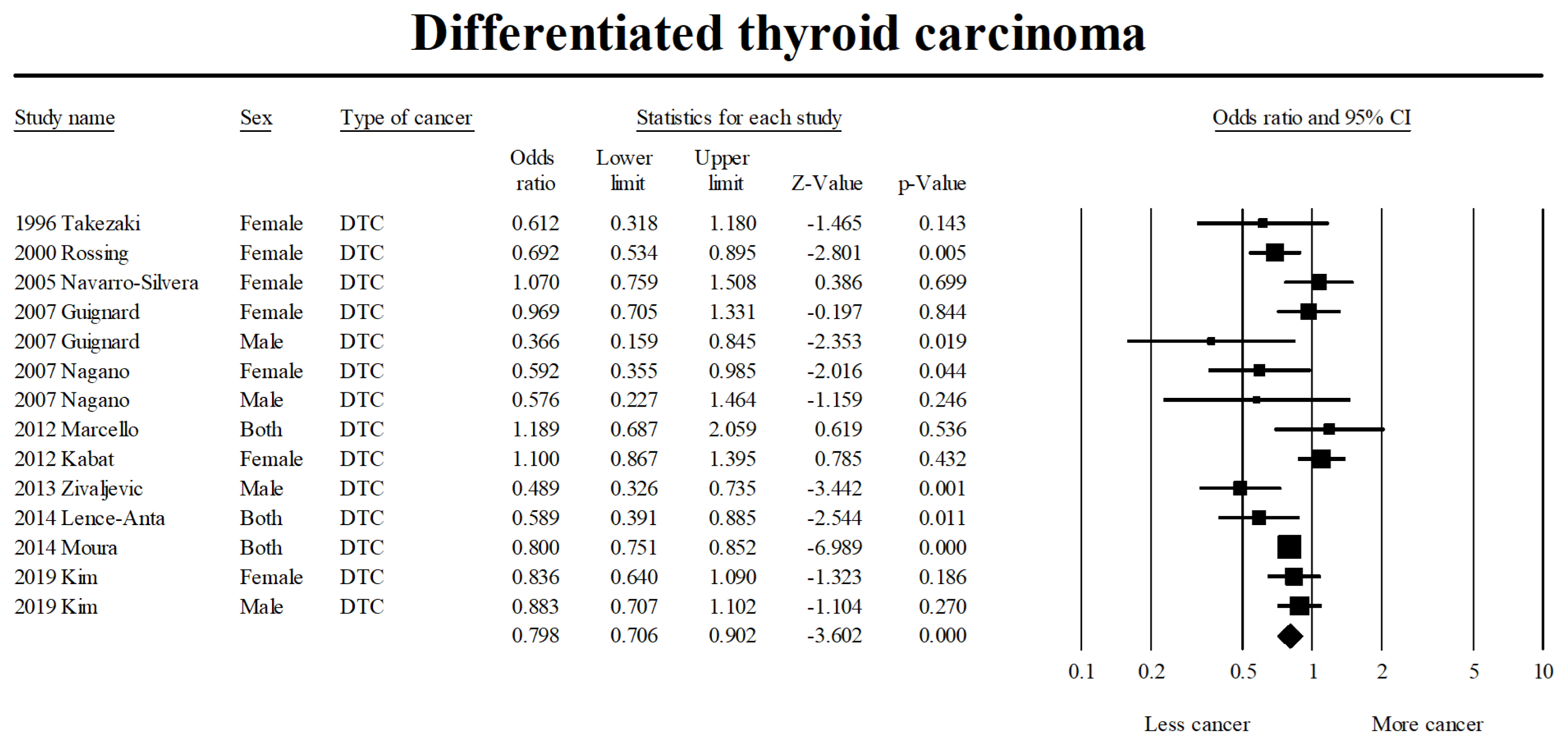
Effect of smoking on differentiated thyroid carcinoma. DTC, differentiated thyroid cancer; CI, confidence interval.
DISCUSSION
This meta-analysis suggests that smoking offers a protective effect against thyroid cancer occurrence. In particular, smokers were less likely to be diagnosed with DTC, which includes papillary thyroid and follicular thyroid carcinomas.
Kitahara et al. [8] reported that current smoking, greater smoking intensity, duration, and pack years were associated with a greater reduction in thyroid cancer risk. By contrast, two large cohort studies conducted in Canada and the USA demonstrated no significant relationship between smoking and thyroid cancer over a median follow-up of 16 to 20 years. These studies, however, were limited as they each had <200 incident thyroid cancers during the follow-up period [5,45].
Cho and Kim [47] conducted a meta-analysis to evaluate smoking and thyroid cancer occurrence using data from 31 studies. This analysis demonstrated a reduced thyroid cancer risk in subjects who had smoked (RR, 0.79; 95% CI, 0.70 to 0.88) compared with those who had never smoked. The results of the current meta-analysis are in agreement with the Cho analysis in that current smokers were less likely to be diagnosed with thyroid cancer. Cho and Kim [47] also demonstrated that papillary thyroid cancers benefited from the protective effect of smoking, as did the current analysis. However, the observation made by Cho and Kim [47] could not be substantiated because only three studies with patients identified as papillary thyroid carcinoma were included in the analysis. The authors acknowledged the possibility of a chance finding due to the small sample size and did not elaborate on this point. By contrast, the analysis reported here substantiates the protective effect of smoking on DTC occurrence by the inclusion of data from 10 studies.
Although the exact mechanism as to how smoking asserts a protective effect on thyroid cancer has not been elucidated, there is a possible connection between the risk of thyroid malignancy and thyroid stimulating hormone (TSH) concentration. According to the Boelaert et al. [48], the risk of malignancy in a thyroid nodule may increase with increasing serum TSH concentrations, even within normal range. A recent study revealed that extracts from cigarette smoking exhibit similar properties to thyroid hormones and can act as partial agonists for thyroid hormone receptors [49]. For smokers, the inhaled cigarette extracts could lead to increases in serum triiodothyronine and thyroxine, which could in turn lead to reduced serum TSH levels [50]. The resulting ‘TSH suppression’ effect would lead to decreased stimulation of the thyroid gland, which may explain why the thyroid cancer, and in particular DTCs, rates are lower in both male and female smokers.
Cigarette smoke exposure is reported to temporarily affect thyroid hormone levels [49]. The protective effect of smoking on thyroid cancer occurrence is lost 3 years after an individual quits smoking [29]. Furthermore, many of the individual studies presented smoking status as current and former smokers. In the current analysis, we did not conduct separate analyses between current and former smokers because the total period of smoking for both groups was not specified in most of the studies.
Our summary results should be interpreted with caution due to the innate limitations of a meta-analysis. First, as a meta-analysis of observational studies that may have inherent limitations, such as bias and uncontrolled cofounding factors, the results may reflect such limitations. Secondly, because our study encompassed many types of studies from different geographic locations and time periods, the Q-statistics and I2 values indicated a high degree of heterogeneity. To address this issue, subgroup analyses were conducted to identify the source of the heterogeneity. Thirdly, cigarette smoking status was assessed based on self-reported questionnaires and the results are difficult to quantify and validate. Likewise, the definition of smoking was not consistent among the studies and the case and control group had to be redefined. Furthermore, gender disparity exists in thyroid cancer and smoking, which is even further complicated by inter-cultural variation of the gender disparity for smoking. With the limited information provided by the individual studies, however, we were not able to adjust for these factors in our subgroup analysis, resulting in a room for selection bias in the process of data extraction.
In conclusion, the results of this meta-analysis reveal that cigarette smoking could be inversely associated with thyroid cancer, which implies a protective effect. Moreover, the association was more pronounced in patients with DTC and was not seen in patients who had quit smoking. However, these data should be interpreted with caution and the fact that smoking is related to many malignancies should be considered. Additional, large, well-designed epidemiological and experimental studies are required to investigate the influence of smoking on the occurrence of thyroid cancer further.
Supplementary Information
PRISMA 2009 Checklist
Notes
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS
Conception or design: J.H.L., Y.J.C., K.H.Y. Acquisition, analysis, or interpretation of data: J.H.L., Y.J.C., K.H.Y. Drafting the work or revising: J.H.L., Y.J.C., K.H.Y. Final approval of the manuscript: J.H.L., Y.J.C., K.H.Y.
Acknowledgements
This research was supported by a grant of Patient-Centered Clinical Research Coordinating Center funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI19-C0481, HC19C0103).