
Articles
- Page Path
- HOME > Endocrinol Metab > Volume 30(1); 2015 > Article
-
Case ReportMultiple Myeloma in a Patient with Acromegaly
- Yu Mi Kang1*, Jong Han Choi1*, Min Jung Lee1, Ari Ahn2, Chan-Jeoung Park2, Kiju Chang3, Seyoung Seo3, Sun In Hong3, Min-Seon Kim1
-
Endocrinology and Metabolism 2015;30(1):110-115.
DOI: https://doi.org/10.3803/EnM.2015.30.1.110
Published online: March 27, 2015
1Division of Endocrinology and Metabolism, Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
2Department of Laboratory Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
3Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- Corresponding author: Min-Seon Kim. Division of Endocrinology and Metabolism, Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Songpa-gu, Seoul 138-736, Korea. Tel: +82-2-3010-3245, Fax: +82-2-3010-6962, mskim@amc.seoul.kr
- *These authors contributed equally to this work.
Copyright © 2015 Korean Endocrine Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
- Acromegaly is a slowly progressing condition resulting from excess growth hormone (GH), generally caused by a GH-secreting pituitary adenoma. Cancer is the third most common cause of mortality in patients with acromegaly, and insulin-like growth factor 1 (IGF-1) is known to influence tumor formation by increasing cell proliferation and inhibiting apoptosis. Multiple myeloma (MM) is a plasma cell neoplasm, and previous studies have suggested the possible role of IGF-1 in its development of MM. However, no cases of acromegaly accompanied with MM have been reported in Asia to date. We here report the case of a 58-year-old woman with acromegaly accompanied with MM who presented with longstanding acromegalic manifestations resulting from a GH-secreting pituitary adenoma and also exhibited anemia, a reversed albumin/globulin ratio, and plasmacytosis on bone marrow examination. Because IGF-1 has been suggested to play an important role in the development and progression of MM, the patient promptly underwent surgical removal of the pituitary adenoma via a transsphenoidal approach. Since there is currently no consensus on therapeutic guidelines and suggested prognosis for MM with acromegaly, long-term follow-up of such cases is needed.
- Acromegaly is a systemic, chronic, and slowly progressing condition resulting from excess growth hormone (GH) and insulin-like growth factor 1 (IGF-1) [1]. It is most commonly caused by a GH-secreting pituitary adenoma [2]. Patients with acromegaly have a 1.6- to 3.3-fold increase in age-related mortality and a 10-year reduction in life expectancy [3], and cancer is the third most common cause of mortality [4]. The role of the GH-IGF-1 axis in the development of malignancy has been continuously investigated, and IGF-1 is thought to enhance cell proliferation and to inhibit apoptosis [4]. Breast cancer is epidemiologically linked to IGF-1 levels in premenopausal women [5], and an increased IGF-1 level may increase the relative risk of developing colon cancer [6].
- Multiple myeloma (MM) is a malignant proliferative disease of monoclonal plasma cells that produce monoclonal immunoglobulins [7]. Diagnosis of MM is made based on the clonal plasmacytosis of at least 15% on bone marrow examination or biopsy-proven clonal plasmacytoma, the presence of M protein in serum or urine, and any evidence of end-organ damage (i.e., hypercalcemia, renal insufficiency, anemia, and bone disease) attributable to myeloma involvement [7].
- Although acromegaly is associated with malignancy, its association with MM has not been thoroughly investigated. Earlier reports demonstrated the role of GH and IGF-1 in B lymphocyte activation [8] and the universal expression of IGF-1 receptors in MM cells in vitro [9]. Also, in several cases, acromegaly was associated with the malignant transformation of monoclonal gammopathy of undetermined significance (MGUS) into overt MM [10,11]. However, only a few actual cases of MM associated with acromegaly have been reported [12,13]. Here we describe the first Asian patient, who was diagnosed with acromegaly and MM, simultaneously.
INTRODUCTION
- A 58-year-old woman was admitted to our department for diagnostic workup of acromegalic features. She had noticed the enlargement of her face, hands, and feet 8 years prior to her visit, and these were associated with hyperhidrosis, a thicker and deeper voice, and decreased libido. At that time, she had also undergone uvulectomy because of obstructive sleep apnea that had caused severe snoring. The snoring continued after surgery, albeit much more infrequently.
- On admission, the patient's blood pressure was 120/80 mm Hg. She had a heart rate of 86 per minute, a respiratory rate of 20 per minute, and a body temperature of 36.5℃. During physical examination, the facial enlargement with frontal bossing was noticed, as was the disproportionate enlargement of the tongue, nose, lips, hands, and feet (Fig. 1). Hypertrichosis was seen, especially in the lower extremities. Soft tissue swelling was noted, and the skin folds were thickened.
- A complete blood count revealed a plasma hemoglobin level of 10.0 g/dL. The serum protein level was 10.5 g/dL (reference range, 6 to 8) and the serum albumin level was 2.5 g/dL (reference range, 3.5 to 5.2), reflecting a reversed albumin/globulin (A/G) ratio. Serum creatinine and calcium levels were 0.63 mg/dL (reference range, 0.70 to 1.40) and 8.6 mg/dL (reference range, 8.6 to 10.2), respectively. Thus, the serum calcium level corrected for hypoalbuminemia was 9.2 mg/dL. The fasting plasma glucose level was 109 mg/dL and the 2-hour postprandial plasma glucose level was 280 mg/dL. Hemoglobin A1c was 7.8% and the C-peptide level was 4.8 ng/mL. The thyroid-stimulating hormone level was 1.5 µU/mL (reference range, 0.4 to 5.0) and the free thyroxine level was 1.3 ng/dL. Basal levels of adrenocorticotropic hormone, prolactin, luteinizing hormone, follicle-stimulating hormone, and estradiol were 23.0 pg/mL, 6.8 ng/mL, 17.1 mIU/mL, 44.4 mIU/mL, and 10.0 pg/mL, respectively, which were all within normal ranges. Serum levels of IGF-1 and human growth hormone (hGH) were elevated to 898 ng/mL (age-adjusted reference range, 71 to 284) and 42 ng/mL (reference range, <16.0), respectively (Tables 1, 2).
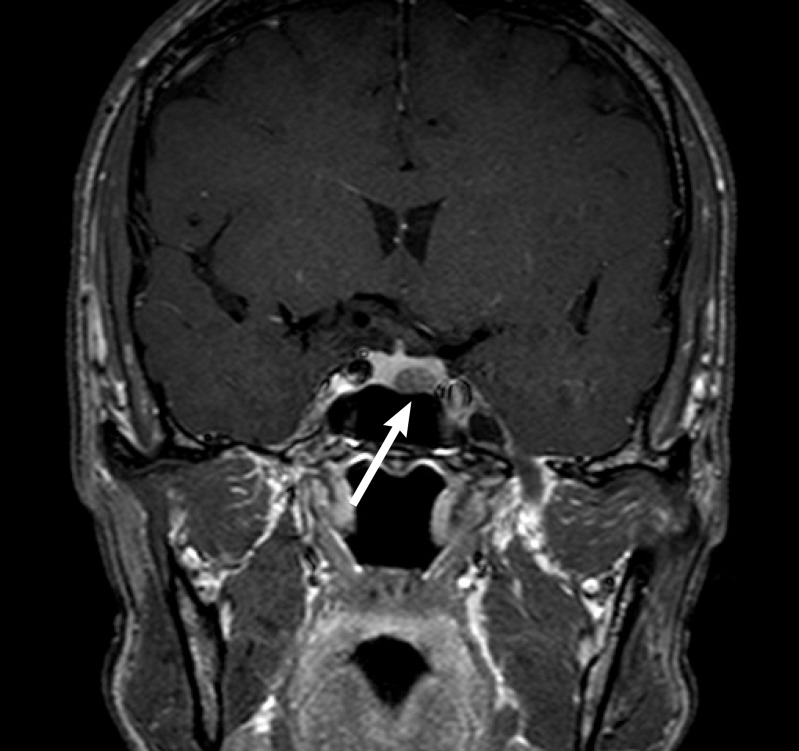
- Because these laboratory findings strongly suggested acromegaly and associated diabetes mellitus, we performed a 75g oral glucose tolerance test (OGTT) to confirm GH hypersecretion (Table 2). To confirm the presence of a GH-secreting pituitary adenoma, we performed magnetic resonance imaging of the sella turcica. It revealed a 1.0×0.6-cm pituitary adenoma on the left side of the pituitary gland (Fig. 2).
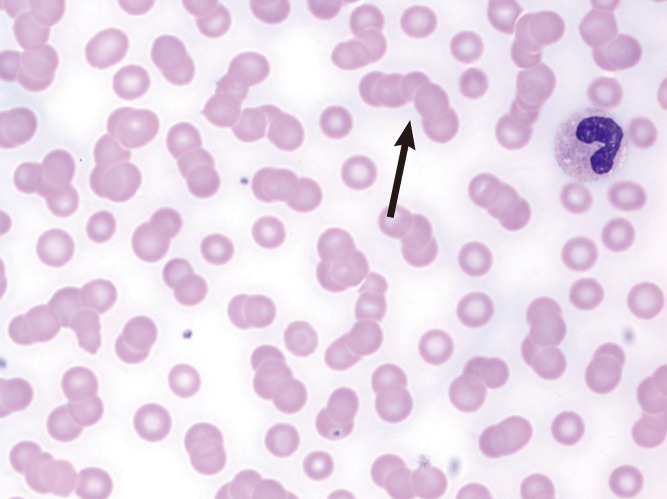
- The markedly reversed A/G ratio and anemia led us to suspect a monoclonal gammopathy such as MM. A peripheral blood smear revealed a red blood cell rouleux formation (Fig. 3). Protein electrophoresis (PEP) and immunofixation electrophoresis (IFE) of serum samples revealed a monoclonal gammopathy (M peak 4.9 g/dL) of immunoglobulin G (IgG)-λ type; PEP and IFE of urine samples were inadequate because of low urinary protein. The patient's serum IgG level was elevated to 5,860.0 mg/dL, and the κ and lambda free light chain ratios were 7.16 and 34.50 mg/L, respectively. To confirm the diagnosis of MM, we performed bone marrow aspiration and biopsy with plasma cell phenotyping. Neoplastic plasma cells were observed on bone marrow aspirate and touchprint slides (Fig. 4A, B), and packed bone marrow with neoplastic plasma cells (35.6% of the clonal plasma cells) was observed in the bone marrow biopsy specimen (Fig. 4C-F). In an attempt to find myeloma-related organ damage, we took simple X-rays of the entire body, and they did not reveal any osteolytic lesions. According to the diagnostic criteria for symptomatic MM, one should exhibit more than one of the parameters reflecting myeloma-related organ dysfunction (Table 3). Because the M peak was >3 g/dL and the proportion of monoclonal plasma cells in the bone marrow was >10% without myeloma-related orgam damages, the patient was diagnosed with asymptomatic (smoldering) MM. However, it is of note that her serum hemoglobin level was at the cutoff value for diagnosis of symptomatic MM and that her serum calcium level was slightly below the cutoff (Table 3). In accordance with the treatment guidelines for asymptomatic MM, we planned close follow-up, with deferral of chemotherapy until the disease became symptomatic.
- To treat the GH-secreting pituitary adenoma, the patient underwent tumor resection via a transsphenoidal approach. There were no immediate postoperative complications. Three days after surgery, the serum IGF-1 level was measured and the 75 g OGTT was repeated. Although the serum hGH level was lower than it had been before surgery, the results indicated incomplete remission immediately after surgery (Table 2). However, after the surgery, the patient exhibited clinical improvements in acromegalic features, such as decreased skin thickness and reduced size of the extremities. She also claimed that the frequency of snoring and daytime drowsiness had decreased dramatically. Therefore, we decided to closely monitor the clinical and biochemical responses to the removal of the GH-secreting pituitary adenoma and to continuously determine the need for further treatment.
CASE REPORT
- Acromegaly is an uncommon endocrinologic disorder caused by overproduction of GH, most commonly by a GH-secreting pituitary adenomas [3]. Earlier epidemiological studies have indicated a possible increase in malignancy risk in patients with acromegaly because GH and IGF-I may promote proliferation and inhibit apoptosis of neoplastic cells [4]. Nabarro [1] found a markedly increased incidence of breast cancer in patients with acromegaly. Also, a large retrospective cohort study conducted by Orme et al. [3] to determine mortality and cancer incidence in 1,362 subjects with acromegaly reported a significant increase in the colon cancer mortality rate and a nonsignificant increase in mortality due to breast cancer. The authors also found that mortality due to all malignant disease and colon cancer increased with higher posttreatment GH levels, which suggests that GH hypersecretion may have modified the progression of coexisting malignancies, particularly colonic carcinomas.
- There have been sporadic case reports of hematologic malignancies such as lymphoma and leukemia associated with acromegaly [12,13]. However, the causal relationship between acromegaly and MM has not been clearly proven in clinical settings. Despite the complexity of the interactions between the bone marrow microenvironment and surrounding stromal cells, attempts have been made to determine the exact mechanisms of GH and IGF-1 in the development and proliferation of myeloma [5,6,14]. Murphy et al. [8] demonstrated that treatment with hGH had stimulatory effects on B-cell proliferation. Georgii-Hemming et al. [9] demonstrated the universal expression of IGF-1 receptors in MM cells and postulated that IGF-1 might act like a growth factor in human MM. Also, Ge and Rudikoff [14] demonstrated a stimulatory effect of IGF-1 on six of eight myeloma cell lines, one of two B lymphoma cell lines, and neither of two T leukemia cell lines, where all cell lines expressed similar levels of IGF-1 receptors. The authors suggested that the IGF-1 pathway is biologically relevant in the later stages of B-cell development.
- There is neither an established therapeutic guideline nor a prognosis specific for acromegaly with MM. However, several cases illustrate that treatment of acromegaly improves the progression of MGUS or MM. Kanazawa et al. [10] reported a case of MGUS in a patient with acromegaly in which the serum IgG level, as well as the GH and IGF-1 levels, decreased after the removal of the GH-secreting pituitary adenoma. Moreover, Tucci et al. [11] described a patient with acromegaly in whom a longstanding MGUS had transformed into overt MM. In this patient, serum and urine M components indicated that MM activity was correlated with serum IGF-1 levels. These findings are solid evidence supporting the hypothesis that elevated GH and IGF-1 levels promote the proliferation of malignant plasma cells in MM and that maintaining low levels of GH and IGF-1 through intensive treatment might be a key therapeutic approach in treating coexistent MM.
- In our case, the patient's serum hemoglobin level (10.0 g/dL) was at the cutoff level for symptomatic MM and her serum calcium level (9.2 mg/dL) was slightly below the cutoff, suggesting that the risk of transformation into symptomatic MM would have been very high had the acromegaly been left untreated. Follow-up measurement of serum and urine M proteins and simultaneous measurement of serum GH levels would be necessary to determine the long-term effect of the removal of the GH-secreting tumor on MM. Although these measurements were unavailable in our study because of the recent diagnosis, we expect a favorable prognosis because of the prompt surgical treatment of the acromegaly before the MM became symptomatic. Likewise, the lack of long-term follow-up data from previously reported cases makes it difficult to predict the prognosis of acromegaly with MM. Further long-term observational studies with a larger data set will allow us to specifically suggest appropriate therapeutic guidelines and to extrapolate the prognosis in patients with acromegaly and MM.
- In summary, this is the first reported case of acromegaly accompanied by MM from Asia. Our case strengthens the hypothesis of prior studies that acromegaly plays a significant role in the development of MM. Considering previous studies that have demonstrated the role of IGF-1 in plasma cell proliferation and the correlation between serum IGF-1 levels and the progression of monoclonal gammopathy, prompt efforts to lower circulating GH and IGF-1 levels are an important therapeutic approach. Further research with a larger set of longer term data is needed to develop treatment guidelines specific for MM accompanying acromegaly and to predict prognosis.
DISCUSSION
-
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
Article information
- 1. Nabarro JD. Acromegaly. Clin Endocrinol (Oxf) 1987;26:481–512. ArticlePubMed
- 2. Freda PU, Post KD. Differential diagnosis of sellar masses. Endocrinol Metab Clin North Am 1999;28:81–117. ArticlePubMed
- 3. Orme SM, McNally RJ, Cartwright RA, Belchetz PE. Mortality and cancer incidence in acromegaly: a retrospective cohort study. United Kingdom Acromegaly Study Group. J Clin Endocrinol Metab 1998;83:2730–2734. PubMed
- 4. Melmed S. Acromegaly and cancer: not a problem? J Clin Endocrinol Metab 2001;86:2929–2934. ArticlePubMed
- 5. Hankinson SE, Willett WC, Colditz GA, Hunter DJ, Michaud DS, Deroo B, Rosner B, Speizer FE, Pollak M. Circulating concentrations of insulin-like growth factor-I and risk of breast cancer. Lancet 1998;351:1393–1396. ArticlePubMed
- 6. Ma J, Pollak MN, Giovannucci E, Chan JM, Tao Y, Hennekens CH, Stampfer MJ. Prospective study of colorectal cancer risk in men and plasma levels of insulin-like growth factor (IGF)-I and IGF-binding protein-3. J Natl Cancer Inst 1999;91:620–625. ArticlePubMedPDF
- 7. Riedel DA, Pottern LM. The epidemiology of multiple myeloma. Hematol Oncol Clin North Am 1992;6:225–247. ArticlePubMed
- 8. Murphy WJ, Rui H, Longo DL. Effects of growth hormone and prolactin immune development and function. Life Sci 1995;57:1–14. ArticlePubMed
- 9. Georgii-Hemming P, Wiklund HJ, Ljunggren O, Nilsson K. Insulin-like growth factor I is a growth and survival factor in human multiple myeloma cell lines. Blood 1996;88:2250–2258. ArticlePubMedPDF
- 10. Kanazawa I, Yamaguchi T, Yamane Y, Murakami N, Kato Y, Sugimoto T. Acromegaly associated with monoclonal gammopathy of undetermined significance (MGUS). Endocr J 2006;53:687–691. ArticlePubMed
- 11. Tucci A, Bonadonna S, Cattaneo C, Ungari M, Giustina A, Guiseppe R. Transformation of a MGUS to overt multiple myeloma: the possible role of a pituitary macroadenoma secreting high levels of insulin-like growth factor 1 (IGF-1). Leuk Lymphoma 2003;44:543–545. ArticlePubMed
- 12. Barbosa FR, Vieira Neto L, Lima GA, Wildemberg LE, Portugal R, Gadelha MR. Hematologic neoplasias and acromegaly. Pituitary 2011;14:377–381. ArticlePubMedPDF
- 13. Hagg E, Asplund K, Holm J. Acromegaly and multiple myeloma. Ann Intern Med 1988;109:437–438. Article
- 14. Ge NL, Rudikoff S. Insulin-like growth factor I is a dual effector of multiple myeloma cell growth. Blood 2000;96:2856–2861. ArticlePubMedPDF
References
(A) Physical examination of the patient revealed frontal bossing, thickened lips, and an enlarged nose. (B) Exaggerated frontal bossing (arrow) observed from the side. Disproportionately enlarged (acromegalic) hands (C) and feet (D) were also seen.

A T1-weighted coronal magnetic resonance imaging of the sella turcica indicated a 10×6-mm hypointense, nonenhanced pituitary adenoma on the left side of the pituitary gland (arrow).
Peripheral blood smear results revealed a red blood cell rouleaux formation (arrow; Wright stain, ×1,000).
(A) Neoplastic plasma cells in the bone marrow aspirate specimen (Wright stain, ×1,000). (B) Numerous clustered neoplastic plasma cells on a bone marrow touchprint slide. (C) Packed neoplastic plasma cells were prominent in a bone marrow biopsy specimen stained with H&E (×400). (D) CD138-positive neoplastic plasma cells in an immunohistochemically stained bone marrow biopsy specimen (×400). In an immunohistochemically stained bone marrow biopsy specimen, neoplastic cells were positive for λ light chain (E, ×400) and negative for κ light chain (F, ×400).

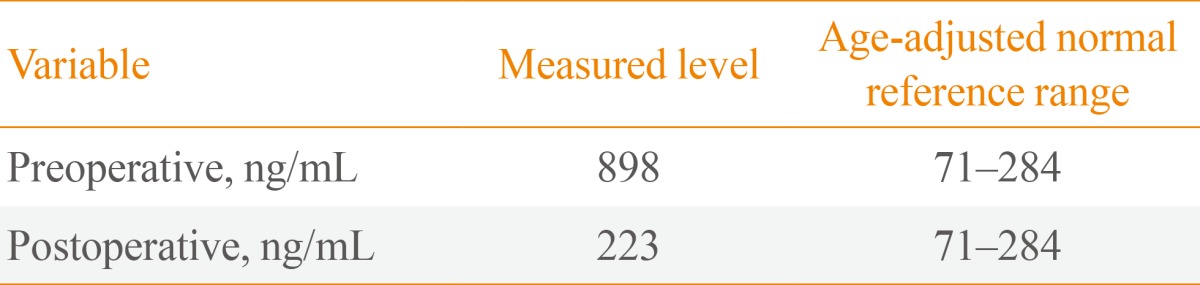
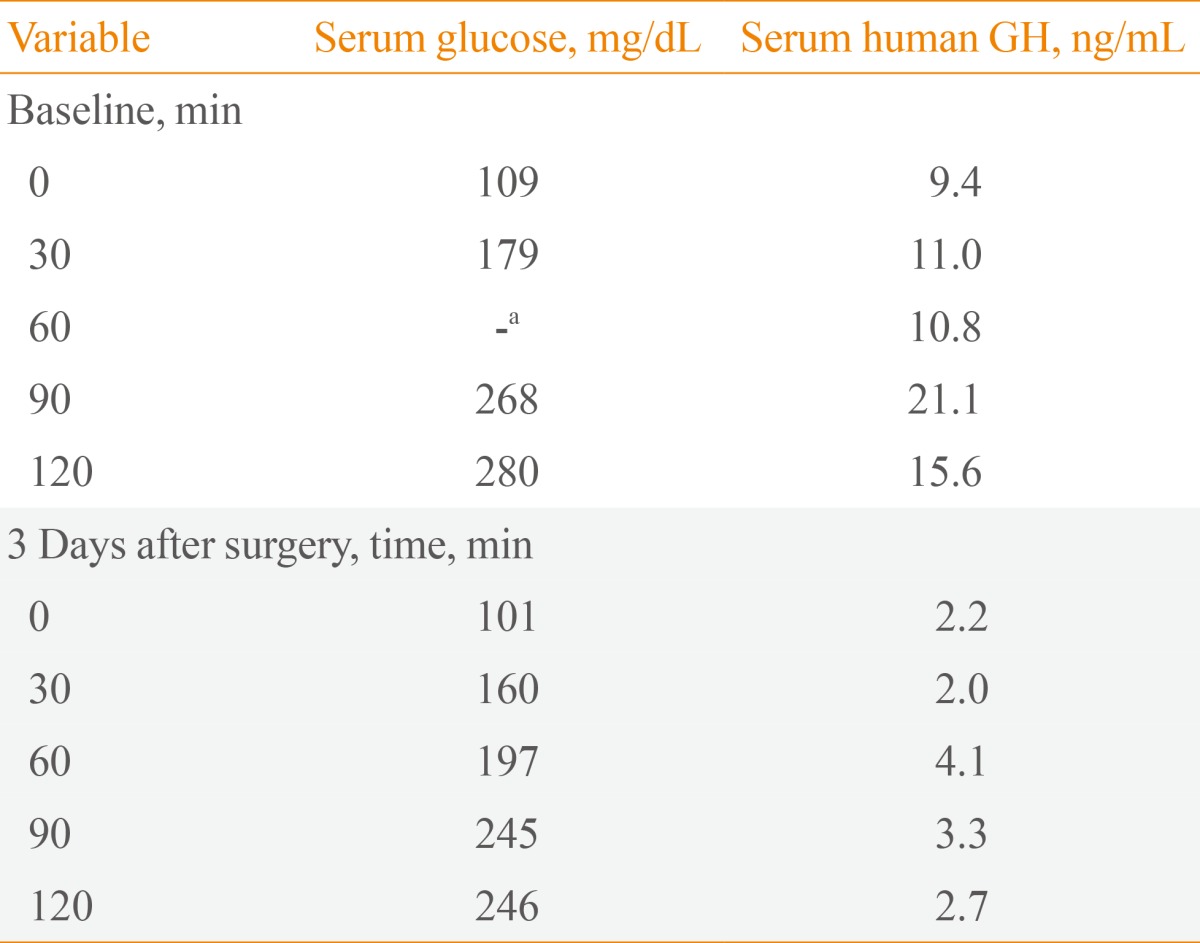

Figure & Data
References
Citations
- Co-Occurrence of Acromegaly and Hematological Disorders: A Myth or Common Pathogenic Mechanism
Prakamya Gupta, Pinaki Dutta
Integrative Medicine International.2017; 4(1-2): 94. CrossRef
 PubReader
PubReader Cite
Cite




