Articles
- Page Path
- HOME > Endocrinol Metab > Volume 32(2); 2017 > Article
-
Original ArticleEffects of Vildagliptin or Pioglitazone on Glycemic Variability and Oxidative Stress in Patients with Type 2 Diabetes Inadequately Controlled with Metformin Monotherapy: A 16-Week, Randomised, Open Label, Pilot Study
-
Nam Hoon Kim1*, Dong-Lim Kim2*, Kyeong Jin Kim1, Nan Hee Kim1, Kyung Mook Choi1, Sei Hyun Baik1, Sin Gon Kim1

-
Endocrinology and Metabolism 2017;32(2):241-247.
DOI: https://doi.org/10.3803/EnM.2017.32.2.241
Published online: June 23, 2017
1Division of Endocrinology and Metabolism, Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea.
2Division of Endocrinology and Metabolism, Department of Internal Medicine, Konkuk University School of Medicine, Seoul, Korea.
- Corresponding author: Sin Gon Kim. Division of Endocrinology and Metabolism, Department of Internal Medicine, Korea University Anam Hospital, Korea University College of Medicine, 73 Inchon-ro, Seongbuk-gu, Seoul 02841, Korea. Tel: +82-2-920-5890, Fax: +82-2-953-9355, k50367@korea.ac.kr
- *These authors contributed equally to this work.
Copyright © 2017 Korean Endocrine Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- Glycemic variability is associated with the development of diabetic complications through the activation of oxidative stress. This study aimed to evaluate the effects of a dipeptidyl peptidase 4 inhibitor, vildagliptin, or a thiazolidinedione, pioglitazone, on glycemic variability and oxidative stress in patients with type 2 diabetes.
-
Methods
- In this open label, randomised, active-controlled, pilot trial, individuals who were inadequately controlled with metformin monotherapy were assigned to either vildagliptin (50 mg twice daily, n=17) or pioglitazone (15 mg once daily, n=14) treatment groups for 16 weeks. Glycemic variability was assessed by calculating the mean amplitude of glycemic excursions (MAGE), which was obtained from continuous glucose monitoring. Urinary 8-iso prostaglandin F2α, serum oxidised low density lipoprotein, and high-sensitivity C-reactive protein were used as markers of oxidative stress or inflammation.
-
Results
- Both vildagliptin and pioglitazone significantly reduced glycated hemoglobin and mean plasma glucose levels during the 16-week treatment. Vildagliptin also significantly reduced the MAGE (from 93.8±38.0 to 70.8±19.2 mg/dL, P=0.046), and mean standard deviation of 24 hours glucose (from 38±17.3 to 27.7±6.9, P=0.026); however, pioglitazone did not, although the magnitude of decline was similar in both groups. Markers of oxidative stress or inflammation including urinary 8-iso prostaglandin F2α did not change after treatment in both groups.
-
Conclusion
- In this 16-week treatment trial, vildagliptin, but not pioglitazone, reduced glycemic variability in individuals with type 2 diabetes who was inadequately controlled with metformin monotherapy, although a reduction of oxidative stress markers was not observed.
- Type 2 diabetes is a chronic metabolic disorder characterised by dysregulated insulin action and hyperglycemia. Lowering serum glucose levels is a mainstay of managing type 2 diabetes in order to reduce the risk of micro- and macrovascular complications [1]. Glycated hemoglobin (HbA1c), time-averaged mean glycemia, is a well-established surrogate marker of long-term glycemia [2]. Most clinical trials of type 2 diabetes, therefore, have focused on lowering serum levels of HbA1c. However, emerging evidence suggests that glycemic variability could contribute to the development of diabetes-related vascular complications, additionally or independently beyond HbA1c [34]. Several studies have indicated that glucose fluctuation is more closely associated with oxidative stress or inflammation than mean glycemia, which has been proposed as a putative mediator of diabetes complications [56].
- On the basis of this evidence, several trials have examined the role of various glucose-lowering agents in the reduction in glycemic variability. For example, acarbose was shown to reduce glucose excursion, measured by mean amplitude of glycemic excursions (MAGE), as well as mean serum glucose in individuals with diabetes [78]. Vildagliptin also reduced MAGE, and was associated with a reduction of markers of oxidative stress or inflammation [69]. On the other hand, the efficacy of agents other than α-glucosidase inhibitor or dipeptidyl peptidase 4 (DPP-4) inhibitor has not been investigated in terms of glycemic variability. Research evidence, however, indicates that pioglitazone, a thiazolidinedione, also possibly contributed to reducing glycemic variability. Pioglitazone reduced glycemic excursion and had a favorable impact on oxidative stress compared to glibenclamide [10].
- Therefore, this study aimed to investigate the effectiveness of different glucose lowering agents, vildagliptin and pioglitazone, on glycemic variability and oxidative stress in patients with type 2 diabetes.
INTRODUCTION
- Study design and population
- A prospective, randomised, open-label, parallel-group, pilot study was performed from September 2008 through January 2015 at the Korea University Anam Hospital and Konkuk University Hospital, Seoul, Korea. The Institutional Review Boards of both Korea University Anam Hospital and Konkuk University Hospital approved the protocol. The trial was registered at ClinicalTrials.gov (NCT01339143).
- Eligible participants were >18 years of age, and diagnosed with type 2 diabetes using American Diabetes Association criteria. All participants had been treated with metformin monotherapy at a stable dose (≥1,000 mg per day) for at least 1 month before randomisation, and had HbA1c of ≥7%, and <10%. Exclusion criteria were type 1 diabetes, uncontrolled hyperglycemia (HbA1c ≥10%), uncontrolled hypertension (systolic blood pressure >160 mm Hg, or diastolic blood pressure >100 mm Hg), symptomatic heart failure, and severe hepatic dysfunction (alanine aminotransferase or aspartate aminotransferase levels more than three times the normal upper limit). Those who had been taking medications affecting oxidative stress markers including a 3-hydroxy-3-methylglutaryl-coenzyme (HMG-CoA) reductase inhibitor, angiotensin-converting enzyme inhibitor, or angiotensin II receptor blocker were not excluded, but were to continue the medications without dose adjustment during the study period. All the individuals provided written informed consent at randomisation.
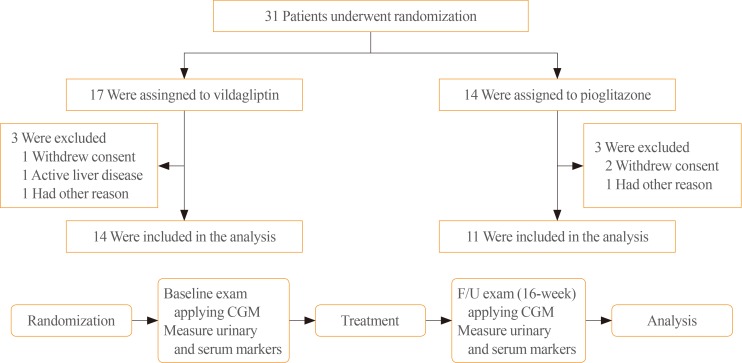
- Of 49 individuals screened, a total of 31 individuals who met the inclusion and exclusion criteria underwent randomisation. Seventeen individuals were assigned to the vildagliptin (50 mg twice daily) group, and 14 individuals to the pioglitazone (15 mg once daily) group. Among them, 25 individuals (n=14 vildagliptin, n=11 pioglitazone) completed the study and were included in the analysis (Fig. 1). At baseline, anthropometric and laboratory measurements were taken after an overnight fast. Height, body weight, and waist circumference were measured, and body mass index (BMI) was calculated. Blood was drawn for biochemical analyses including fasting plasma glucose (FPG), HbA1c, total cholesterol, triglyceride, high density lipoprotein cholesterol, low density lipoprotein (LDL) cholesterol, liver enzymes, and creatinine. C-peptide and insulin were also measured using radioimmunoassay (GammaPro, Seyoung NDC Ltd., Seoul, Korea). A continuous glucose monitoring (CGM) system for measurement of glycemic variability was applied to all participants at baseline and at the final visit. Urine and serum measurements of oxidative stress and inflammatory markers were also taken at the same time.
- The primary outcome was a change in glycemic variability measured by MAGE from baseline to week 16 in each treatment arm. Secondary outcomes were changes in oxidative stress and inflammatory markers, FPG, and HbA1c from baseline to week 16.
- Continuous subcutaneous glucose monitoring and assessment of glycemic variability
- All individuals underwent continuous subcutaneous glucose monitoring (Medtronic, Minneapolis, MN, USA) for 3 consecutive days at the first and last visits. The sensor was inserted on day 1 and removed on day 3 at both visits. Subcutaneous interstitial glucose levels were measured every 5 minutes and automatically stored in the software program. On day 2, a standardised meal was provided to all participants, and venous sampling for FPG was performed for calibration.
- The MAGE was measured in a standardised manner proposed by Service et al. [11]. MAGE is defined as the average height of glucose excursions (peak to nadir, or nadir to peak) that exceeds one standard deviation (SD) for a day. A numerical value of SD was used provided by 24 hours CGM data as an additional marker of glycemic variability [12].
- Oxidative stress and inflammatory markers
- For the measurement of urinary 8-iso prostaglandin F2α (8-iso PGF2α), three consecutive first voided urine samples during applying CMG were used. Samples were measured by Spetramax 190 enzyme-linked immunosorbent assay (ELISA) kit (Cell Biolabs, Seoul, Korea). The intra-assay coefficient of variation was 5.3%. Commercially available ELISAs were also used to measure plasma oxidised LDL (Mercodia Co., Uppsala, Sweden), and high-sensitivity C-reactive protein (hsCRP) (Roche Diagnostics, Indianapolis, IN, USA). The intra-assay coefficient of variation was 7.8% for oxidised LDL, and 9.1% for hsCRP.
- Statistical analysis
- For data summaries, continuous variables were summarised using the mean±SD. Categorical variables were summarised using frequency counts and percentages. The baseline characteristics were compared between groups using Mann-Whitney test for continuous variables, and Fisher exact test for categorical variables. For the analyses of the primary and secondary outcomes, a Wilcoxon signed rank test was performed. Statistical significance was assessed based on a two-sided 5% level of significance, and all statistical analyses were performed using SAS version 9.3 (SAS Institute, Cary, NC, USA).
METHODS
- Baseline characteristics of participants in both the vildagliptin (n=14) and pioglitazone (n=11) groups are presented in Table 1. The mean age was 56.4±11.1 years, and the mean BMI was 26.2±3.4 kg/m2 in all participants. All clinical and anthropometric variables were comparable between groups. Baseline HbA1c (7.2% vs. 7.4%), insulin, and C-peptide levels were also not different between study groups. Markers of glycemic variability including MAGE, SD of 24 hours glucose, and the difference between maximum and minimum glucose levels (Δglucose, max-min) were measured via CGM during 3 consecutive days. Their mean values were similar in both groups.
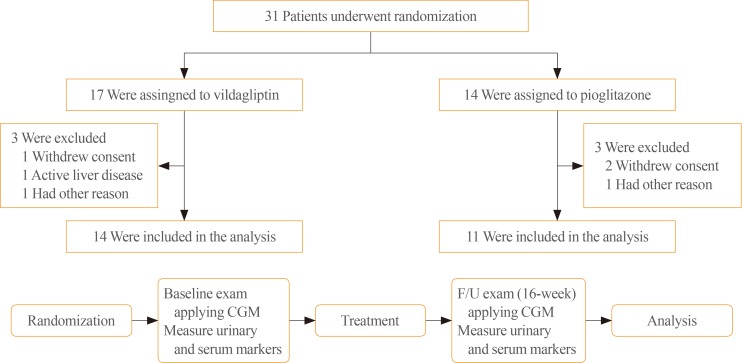
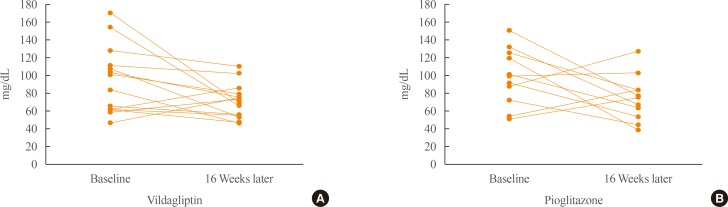
- During the 16-week treatment period, both treatments significantly lowered mean HbA1c (7.2% to 6.4%, P=0.001 in the vildagliptin group; 7.4% to 6.7%, P=0.005 in the pioglitazone group), and 24-hour mean glucose (160.9 to 122.9 mg/dL, P=0.001 and 145.0 to 125.9 mg/dL, P=0.012, respectively) (Table 2). Only vildagliptin treatment, however, significantly reduced markers of glycemic variability including MAGE (P=0.046), SD of 24 hours glucose (P=0.026), and Δglucose, max-min (P=0.036) (Table 2, Fig. 2). Although it was not significant, the magnitude of decline of MAGE in the pioglitazone group was similar to that in the vildagliptin group; hence, each individual's change of MAGE was assessed in both groups (Fig. 3). A more consistent decline of MAGE was found in the vildagliptin group than in the pioglitazone group. In the vildagliptin group, the MAGE value was increased in only two of 14 individuals, but four of 11 individuals in pioglitazone group.
- Finally, oxidative stress markers were measured, but both treatments did not change urinary 8-iso PGF2α (Table 3). Oxidised LDL and hsCRP were also not changed after either treatment.
RESULTS
- In this 16-week randomised controlled trial, vildagliptin, but not pioglitazone, reduced glycemic variability in individuals with type 2 diabetes inadequately controlled with metformin. Vildagliptin significantly reduced markers of glycemic variability including MAGE, SD of 24 hours glucose measured by CGM, as well as HbA1c, and FPG. The attenuated glucose excursion in a glucose-dependent manner with DPP-4 inhibition may contribute to the reduction of glycemic variability markers. Pioglitazone also was effective in lowering HbA1c, but did not reduce glycemic variability.
- Since it has been suggested that glycemic variability contributes to the development of diabetic vascular complications in addition to long-term glycemia [413], some trials have examined the role of pharmacologic interventions in reducing glycemic variability in individuals with diabetes. Most of the trials focused on glucose-lowering medications which mainly acts to reduce postprandial hyperglycemia, such as the α-glucosidase inhibitor [8], DPP-4 inhibitor [6914], and rapid-acting insulin analogues [15]. In short-term clinical studies, the DPP-4 inhibitors, vildagliptin and sitagliptin, effectively reduced MAGE and other glycemic variability markers [914]. Notably, in a comparative study, vildagliptin was superior to sitagliptin in reducing glycemic variability, and was associated with reduction of oxidative stress, which was suggested as a possible link between glycemic variability and vascular complications [6]. The results from the present study are consistent with previous vildagliptin studies in terms of reducing glycemic variability. However, we did not observe the significant effects of vildagliptin on oxidative stress. This outcome was probably due to a small sample size, or a difference in oxidative stress markers. On the other hand, it is also possible that the reduction in glycemic variability does not necessarily lead to reduction of oxidative stress. In this study, overall decreasing trends of urinary 8-iso PGF2α were not observed after vildagliptin treatments in 14 individuals. In addition, the absence of a correlation between glycemic variability and oxidative stress has already been reported in previous several studies. For example, sitagliptin treatment for 4 weeks significantly reduced the MAGE; however, it was not associated with a reduction in oxidative stress markers [14]. In another study, there was no relationship between glucose variability and urinary 15(S)-8-iso PGF2α in individuals with type 1 diabetes [16]. Although it is well established that glucose fluctuation leads to the generation of oxidative stress and endothelial dysfunction, a condition that underlies development of diabetes complications [51718], additional clinical evidence is needed in order to demonstrate that interventions reducing glycemic variability would prevent oxidative stress and the development of further vascular damage.
- We also evaluated the effects of a thiazolidinedione pioglitazone on glycemic variability. This is the first study to measure changes of MAGE after pioglitazone treatment. According to clinical evidence, pioglitazone effectively reduced postprandial glucose excursion and circulating levels of oxidative stress or proinflammatory markers in type 2 individuals with diabetes [1019]. However, whether those effects were accompanied by a reduction in glycemic variability was not clear. In the present study, we found that pioglitazone treatment during 16 weeks did not exert beneficial effects on either glycemic variability or oxidative stress, although it significantly decreased mean glycemia (HbA1c). Therefore, the finding a thiazolidinedione reduced glucose-induced oxidative stress via AMP-activated protein kinase-dependent mechanism seemed to be its own effect in response to hyperglycemia [20], not by preventing glucose fluctuation.
- This study had the following limitations. First, the number of participants was small. We should not overlook the findings that absolute magnitude of decrease in mean value of MAGE was similar between pioglitazone and vildagliptin groups; however, statistically significant change was observed only in vildagliptin group. The interpretation of these findings might be limited by small sample size. Second, the study duration might be short assessing the full glucose-lowering effects of study drugs. So, a larger scale, longer-term study is still warranted to assess the role pharmacologic interventions in terms of glycemic variability. Third, the dose of pioglitazone was 15 mg per day, not 30 mg as used in previous studies, due to insurance criteria in Korea. It might produce smaller effect on glycemic control and variability than expected.
- In conclusion, this study found that a 16-week treatment using vildagliptin, not pioglitazone, reduced glycemic variability in individuals with type 2 diabetes that was inadequately controlled with metformin monotherapy, although oxidative stress markers did not improve. The study identified that DPP-4 inhibitors might have a beneficial role in reducing glycemic variability beyond reducing mean glycemia in individuals with type 2 diabetes.
DISCUSSION
-
Acknowledgements
- This study was undertaken as an investigator-initiated research protocol and was funded by Novartis Korea. Dr. Sin Gon Kim also was partly supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare, Republic of Korea (grant number: HI14C2750). We acknowledge the investigators and staff, as well as study participants.
ACKNOWLEDGMENTS
-
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
Article information
- 1. Stratton IM, Adler AI, Neil HA, Matthews DR, Manley SE, Cull CA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ 2000;321:405–412. ArticlePubMedPMC
- 2. Koenig RJ, Peterson CM, Jones RL, Saudek C, Lehrman M, Cerami A. Correlation of glucose regulation and hemoglobin AIc in diabetes mellitus. N Engl J Med 1976;295:417–420. ArticlePubMed
- 3. Hirsch IB, Brownlee M. Should minimal blood glucose variability become the gold standard of glycemic control? J Diabetes Complications 2005;19:178–181. ArticlePubMed
- 4. Brownlee M, Hirsch IB. Glycemic variability: a hemoglobin A1c-independent risk factor for diabetic complications. JAMA 2006;295:1707–1708. ArticlePubMed
- 5. Monnier L, Mas E, Ginet C, Michel F, Villon L, Cristol JP, et al. Activation of oxidative stress by acute glucose fluctuations compared with sustained chronic hyperglycemia in patients with type 2 diabetes. JAMA 2006;295:1681–1687. ArticlePubMed
- 6. Rizzo MR, Barbieri M, Marfella R, Paolisso G. Reduction of oxidative stress and inflammation by blunting daily acute glucose fluctuations in patients with type 2 diabetes: role of dipeptidyl peptidase-IV inhibition. Diabetes Care 2012;35:2076–2082. ArticlePubMedPMC
- 7. Shimabukuro M, Higa N, Chinen I, Yamakawa K, Takasu N. Effects of a single administration of acarbose on postprandial glucose excursion and endothelial dysfunction in type 2 diabetic patients: a randomized crossover study. J Clin Endocrinol Metab 2006;91:837–842. ArticlePubMed
- 8. McCulloch DK, Kurtz AB, Tattersall RB. A new approach to the treatment of nocturnal hypoglycemia using alpha-glucosidase inhibition. Diabetes Care 1983;6:483–487. ArticlePubMed
- 9. Marfella R, Barbieri M, Grella R, Rizzo MR, Nicoletti GF, Paolisso G. Effects of vildagliptin twice daily vs. sitagliptin once daily on 24-hour acute glucose fluctuations. J Diabetes Complications 2010;24:79–83. ArticlePubMed
- 10. Mori Y, Itoh Y, Obata T, Tajima N. Effects of pioglitazone vs glibenclamide on postprandial increases in glucose and triglyceride levels and on oxidative stress in Japanese patients with type 2 diabetes. Endocrine 2006;29:143–148. ArticlePubMed
- 11. Service FJ, Molnar GD, Rosevear JW, Ackerman E, Gatewood LC, Taylor WF. Mean amplitude of glycemic excursions, a measure of diabetic instability. Diabetes 1970;19:644–655. ArticlePubMed
- 12. Service FJ. Glucose variability. Diabetes 2013;62:1398–1404. ArticlePubMedPMC
- 13. Nalysnyk L, Hernandez-Medina M, Krishnarajah G. Glycaemic variability and complications in patients with diabetes mellitus: evidence from a systematic review of the literature. Diabetes Obes Metab 2010;12:288–298. ArticlePubMed
- 14. Kim HS, Shin JA, Lee SH, Kim ES, Cho JH, Son HY, et al. A comparative study of the effects of a dipeptidyl peptidase-IV inhibitor and sulfonylurea on glucose variability in patients with type 2 diabetes with inadequate glycemic control on metformin. Diabetes Technol Ther 2013;15:810–816. ArticlePubMed
- 15. Anderson JH Jr, Brunelle RL, Keohane P, Koivisto VA, Trautmann ME, Vignati L, et al. Mealtime treatment with insulin analog improves postprandial hyperglycemia and hypoglycemia in patients with non-insulin-dependent diabetes mellitus. Multicenter Insulin Lispro Study Group. Arch Intern Med 1997;157:1249–1255. ArticlePubMed
- 16. Wentholt IM, Kulik W, Michels RP, Hoekstra JB, DeVries JH. Glucose fluctuations and activation of oxidative stress in patients with type 1 diabetes. Diabetologia 2008;51:183–190. ArticlePubMedPDF
- 17. Ceriello A, Esposito K, Piconi L, Ihnat MA, Thorpe JE, Testa R, et al. Oscillating glucose is more deleterious to endothelial function and oxidative stress than mean glucose in normal and type 2 diabetic patients. Diabetes 2008;57:1349–1354. ArticlePubMed
- 18. Standl E, Schnell O, Ceriello A. Postprandial hyperglycemia and glycemic variability: should we care? Diabetes Care 2011;34(Suppl 2):S120–S127. ArticlePubMedPMC
- 19. Agarwal R. Anti-inflammatory effects of short-term pioglitazone therapy in men with advanced diabetic nephropathy. Am J Physiol Renal Physiol 2006;290:F600–F605. ArticlePubMed
- 20. Ceolotto G, Gallo A, Papparella I, Franco L, Murphy E, Iori E, et al. Rosiglitazone reduces glucose-induced oxidative stress mediated by NAD(P)H oxidase via AMPK-dependent mechanism. Arterioscler Thromb Vasc Biol 2007;27:2627–2633. ArticlePubMed
References
Changes of (A) mean amplitude of glycemic excursion (MAGE) and (B) standard deviation (SD) before and after 16 weeks of treatment in the vildagliptin and pioglitazone groups. aP<0.05.

Changes of mean amplitude of glycemic excursion before and after 16 weeks of treatment in the (A) vildagliptin and (B) pioglitazone groups on individual levels.
Baseline Characteristics of the Study Subjects
Values are expressed as number (%) or mean±SD.
HbA1c, glycated hemoglobin; LDL-C, low density lipoprotein cholesterol; HDL-C, high density lipoprotein cholesterol; ARB, angiotensin II receptor blocker; ACE, angiotensin-converting enzyme; SD, standard deviation; MAGE, mean amplitude of glycemic excursion.
aFrom continuous glucose monitoring system measurements over a 24-hour period; bDifference between maximum and minimum glucose.
Fasting Plasma Glucose, HbA1c, and Markers of Glycemic Variability before and after Treatments (16 Weeks) in Vildagliptin and Pioglitazone Group
Changes of Oxidative Stress Markers before and after Treatments (16 Weeks) in Vildagliptin and Pioglitazone Group
Figure & Data
References
Citations
- What is Glycaemic Variability and which Pharmacological Treatment Options are Effective? A Narrative Review
Juan Miguel Huertas Cañas, Maria Alejandra Gomez Gutierrez, Andres Bedoya Ossa
European Endocrinology.2023; 19(2): 4. CrossRef - Glycemic Variability, Glycated Hemoglobin, and Cardiovascular Complications: Still a Dilemma in Clinical Practice
Antonio Ceriello, Ali A. Rizvi, Manfredi Rizzo
Advances in Therapy.2022; 39(1): 1. CrossRef - Contrasting Three Non-hypoglycemic Antidiabetic Drug Effects on Glycemic Control in Newly Diagnosed Type II Diabetes Mellitus: An Experimental Study
Abdulhamza Hmood, Mohammed Almasoody, Hameed Hussein Al-Jameel
Open Access Macedonian Journal of Medical Sciences.2022; 10(B): 506. CrossRef - Hypoglycemic agents and glycemic variability in individuals with type 2 diabetes: A systematic review and network meta-analysis
SuA Oh, Sujata Purja, Hocheol Shin, Minji Kim, Eunyoung Kim
Diabetes and Vascular Disease Research.2022; 19(3): 147916412211068. CrossRef - Influence of dipeptidyl peptidase-4 inhibitors on glycemic variability in patients with type 2 diabetes: A meta-analysis of randomized controlled trials
Shangyu Chai, Ruya Zhang, Ye Zhang, Richard David Carr, Yiman Zheng, Swapnil Rajpathak, Miao Yu
Frontiers in Endocrinology.2022;[Epub] CrossRef - Comparison of Efficacy of Glimepiride, Alogliptin, and Alogliptin-Pioglitazone as the Initial Periods of Therapy in Patients with Poorly Controlled Type 2 Diabetes Mellitus: An Open-Label, Multicenter, Randomized, Controlled Study
Hae Jin Kim, In Kyung Jeong, Kyu Yeon Hur, Soo-Kyung Kim, Jung Hyun Noh, Sung Wan Chun, Eun Seok Kang, Eun-Jung Rhee, Sung Hee Choi
Diabetes & Metabolism Journal.2022; 46(5): 689. CrossRef - Effect of low dose allopurinol on glycemic control and glycemic variability in patients with type 2 diabetes mellitus: A cross-sectional study
Manal M. Alem
Heliyon.2022; 8(11): e11549. CrossRef - Effect of hydroxychloroquine on glycemic variability in type 2 diabetes patients uncontrolled on glimepiride and metformin therapy
Rajesh Rajput, Suyasha Saini, Siddhant Rajput, Parankush Upadhyay
Indian Journal of Endocrinology and Metabolism.2022; 26(6): 537. CrossRef - Effect of Dapagliflozin as an Add-on Therapy to Insulin on the Glycemic Variability in Subjects with Type 2 Diabetes Mellitus (DIVE): A Multicenter, Placebo-Controlled, Double-Blind, Randomized Study
Seung-Hwan Lee, Kyung-Wan Min, Byung-Wan Lee, In-Kyung Jeong, Soon-Jib Yoo, Hyuk-Sang Kwon, Yoon-Hee Choi, Kun-Ho Yoon
Diabetes & Metabolism Journal.2021; 45(3): 339. CrossRef - Comprehensive elaboration of glycemic variability in diabetic macrovascular and microvascular complications
Bao Sun, Zhiying Luo, Jiecan Zhou
Cardiovascular Diabetology.2021;[Epub] CrossRef - CGMS and Glycemic Variability, Relevance in Clinical Research to Evaluate Interventions in T2D, a Literature Review
Anne-Esther Breyton, Stéphanie Lambert-Porcheron, Martine Laville, Sophie Vinoy, Julie-Anne Nazare
Frontiers in Endocrinology.2021;[Epub] CrossRef - Efficacy and safety profile of sitagliptin, vildagliptin, and metformin in newly diagnosed type 2 diabetic subjects
Sahar Hossam Elhini, Amal K. Hussien, Ahmed Abd Elsamie Omran, Asmaa A. Elsayed, Haitham saeed
Clinical and Experimental Pharmacology and Physiology.2021; 48(12): 1589. CrossRef - Vildagliptin ameliorates renal injury in type 2 diabetic rats by suppressing oxidative stress
Fariba Aghahoseini, Alireza Alihemmati, Leila Hosseini, Reza Badalzadeh
Journal of Diabetes & Metabolic Disorders.2020; 19(2): 701. CrossRef - Small changes in glucose variability induced by low and high glycemic index diets are not associated with changes in β-cell function in adults with pre-diabetes
Kristina M. Utzschneider, Tonya N. Johnson, Kara L. Breymeyer, Lisa Bettcher, Daniel Raftery, Katherine M. Newton, Marian L. Neuhouser
Journal of Diabetes and its Complications.2020; 34(8): 107586. CrossRef - Comparison of the effects of gemigliptin and dapagliflozin on glycaemic variability in type 2 diabetes: A randomized, open‐label, active‐controlled, 12‐week study (STABLE II study)
Soo Heon Kwak, You‐Cheol Hwang, Jong Chul Won, Ji Cheol Bae, Hyun Jin Kim, Sunghwan Suh, Eun Young Lee, Subin Lee, Sang‐Yong Kim, Jae Hyeon Kim
Diabetes, Obesity and Metabolism.2020; 22(2): 173. CrossRef - Glycemic variability: adverse clinical outcomes and how to improve it?
Zheng Zhou, Bao Sun, Shiqiong Huang, Chunsheng Zhu, Meng Bian
Cardiovascular Diabetology.2020;[Epub] CrossRef - Anti-inflammatory properties of antidiabetic drugs: A “promised land” in the COVID-19 era?
Niki Katsiki, Ele Ferrannini
Journal of Diabetes and its Complications.2020; 34(12): 107723. CrossRef - Impact of long-term glucose variability on coronary atherosclerosis progression in patients with type 2 diabetes: a 2.3 year follow-up study
Suhua Li, Xixiang Tang, Yanting Luo, Bingyuan Wu, Zhuoshan Huang, Zexiong Li, Long Peng, Yesheng Ling, Jieming Zhu, Junlin Zhong, Jinlai Liu, Yanming Chen
Cardiovascular Diabetology.2020;[Epub] CrossRef - Visit-to-visit fasting plasma glucose variability is an important risk factor for long-term changes in left cardiac structure and function in patients with type 2 diabetes
Xixiang Tang, Junlin Zhong, Hui Zhang, Yanting Luo, Xing Liu, Long Peng, Yanling Zhang, Xiaoxian Qian, Boxiong Jiang, Jinlai Liu, Suhua Li, Yanming Chen
Cardiovascular Diabetology.2019;[Epub] CrossRef - Effect of dipeptidyl-peptidase-4 inhibitors on C-reactive protein in patients with type 2 diabetes: a systematic review and meta-analysis
Xin Liu, Peng Men, Bo Wang, Gaojun Cai, Zhigang Zhao
Lipids in Health and Disease.2019;[Epub] CrossRef - Efficacy and Safety of Pioglitazone Monotherapy in Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomised Controlled Trials
Fahmida Alam, Md. Asiful Islam, Mafauzy Mohamed, Imran Ahmad, Mohammad Amjad Kamal, Richard Donnelly, Iskandar Idris, Siew Hua Gan
Scientific Reports.2019;[Epub] CrossRef - Effect of DPP-IV Inhibitors on Glycemic Variability in Patients with T2DM: A Systematic Review and Meta-Analysis
Subin Lee, Heeyoung Lee, Yoonhye Kim, EunYoung Kim
Scientific Reports.2019;[Epub] CrossRef - Glycemic Variability: How to Measure and Its Clinical Implication for Type 2 Diabetes
Guillermo E. Umpierrez, Boris P. Kovatchev
The American Journal of the Medical Sciences.2018; 356(6): 518. CrossRef
 PubReader
PubReader Cite
Cite