Associations of Perirenal Fat Thickness with Renal and Systemic Calcified Atherosclerosis
Article information

Abstract
Background
We investigated associations between perirenal fat thickness and atherosclerotic calcification in six different vascular beds.
Methods
Using a community-based cohort (n=3,919), perirenal fat thickness was estimated from computed tomography scans. It was classified as Q1 (the lowest quartile) to Q4 (the highest quartile) in each sex. Calcification in the carotid arteries, coronary arteries, thoracic aorta, abdominal aorta, iliac arteries, and renal arteries was evaluated.
Results
Perirenal fat thickness was associated with older age (P<0.01) and a higher prevalence of obesity, hypertension, and dyslipidemia (P<0.01 for all). Perirenal fat thickness was independently associated with renal arterial calcification even after adjustment for age, sex, body mass index, hypertension, dyslipidemia, smoking history, and family history of heart diseases in first-degree relatives (odds ratio [OR] per quartile of perirenal fat thickness, 1.25; 95% confidence interval [CI], 1.09 to 1.44). Compared to Q1, the odds of renal arterial calcification in Q4 was about two times higher (OR, 2.05; 95% CI, 1.29 to 3.25). After adjustment for renal arterial calcification and atherosclerotic risk factors, the only other vascular bed where perirenal fat thickness showed a significant association with calcification was the abdominal aorta (OR, 1.11; 95% CI, 1.00 to 1.23; P=0.045).
Conclusion
Perirenal fat thickness was independently associated with vascular calcification in the renal artery and abdominal aorta.
INTRODUCTION
Visceral fat, intrahepatic fat, and intramuscular fat are involved in lipid and glucose metabolism and contribute to the development of metabolic abnormalities [12345]. They also cause lipotoxicity and inflammation [678], and consequently, atherosclerosis [18910].
Perirenal fat has the same developmental origins as visceral fat [11]. It is associated not only with waist circumference and metabolic syndrome [12], but also with the risk of hypertension [13] and chronic kidney disease [14]. However, few studies have investigated the association between perirenal fat thickness and systemic atherosclerosis. In addition, since renal sinus fat has been reported to exert a local effect on the renin-angiotensin-aldosterone system [1516], perirenal fat might have different associations with atherosclerosis in other arterial beds depending on their location.
Perirenal fat thickness was assessed by computed tomography (CT), which has been reported to be a reliable method of measuring perirenal fat volume [17]. In the current study, we investigated the association between perirenal fat thickness and arterial calcification using a large community-based cohort that was evaluated for the extent of calcified atherosclerosis in six different vascular beds: the carotid arteries, coronary arteries, thoracic aorta, abdominal aorta, iliac arteries, and renal arteries. In addition, differences in the association between perirenal fat and vascular calcification among different arterial beds were evaluated.
METHODS
Study population
From October 1999 to July 2003, 9,763 asymptomatic subjects visited a university-affiliated disease prevention center in San Diego, California and had a CT scan for preventive health screening [10]. Most subjects were self-referred or referred by their primary care provider. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki and was reviewed and approved by the Institutional Review Board (IRB) of the University of California, San Diego, Human Research Protections Program (IRB number: 150603). All subjects provided informed consent.
For the current study, we analyzed subjects who had CT scans of the carotid arteries, coronary arteries, thoracic aorta, abdominal aorta, iliac arteries, and renal arteries (n=4,671). To minimize confounders between ectopic fat and systemic atherosclerosis, subjects with diabetes mellitus [18] or a history of coronary bypass, cardiac or carotid stent, or stroke were excluded (n=577). After additionally excluding subjects with intra-abdominal masses on their CT scans (n=98) or with a poor-quality CT scan in terms of perirenal fat on both sides (n=77), 3,919 subjects were included in the analysis.
Clinical and laboratory assessments
Before undergoing the scanning procedure, a questionnaire was used to obtain medical history, current medications, smoking history, and family history of cardiovascular diseases. Height and weight were measured using a stadiometer and standardized scale. From these measurements, body mass index (BMI) was calculated as kilograms divided by meters squared (kg/m2) and obesity was defined as a BMI ≥30 kg/m2 [19]. Systolic and diastolic blood pressure measurements were obtained by a trained technician after the participant rested for 5 minutes. Hypertension was defined as systolic blood pressure >140 mm Hg, diastolic blood pressure >90 mm Hg, or the use of anti-hypertensive medications. Casual serum lipid and glucose levels were obtained via a finger-stick using the Cholestech LDX system (Alere, Hayward, CA, USA). Dyslipidemia was defined as a ratio of total to high-density lipoprotein cholesterol (HDL-C) of >5, or the use of cholesterol-lowering medication. Diabetes mellitus was identified by the current use of anti-diabetic medications or a casual serum glucose level ≥200 mg/dL. Smoking status was classified as current smokers, ex-smokers, and never-smokers.
Imaging
The determination of quantitative calcium scores in various arterial beds has been described previously [10202122]. Briefly, all participants underwent imaging with an Imatron C-150 scanner (GE Imatron, San Francisco, CA, USA). Each bed was obtained by a distinct scan of the segment in question using the following slice thicknesses: 3 mm for the coronary bed; 6 mm through the neck, abdomen, and pelvis; and 5 mm for the thorax. Cardiac tomographic imaging was performed with electrocardiogram-gated triggering. The coronary artery calcium score was calculated according to the method described by Agatston et al. [23]. Atherosclerotic calcification was defined as a plaque of ≥2 pixels (area=0.67 mm2) with a density of ≥130 Hounsfield units. Data from the left and right sides were combined to give the extent of calcium in the carotid, iliac, and renal arterial beds.
On CT scans, perirenal fat thickness was evaluated as the distance from the kidney to the nearest viscera or muscle, and five perirenal measurements were taken (medial, posterior, lateral, anterolateral, and posterolateral) on a slice passing through the renal vein (Supplemental Fig. S1) [172425]. All five measurements were made on both sides for each patient. One reader measured the scans blinded to the demographic data. The reproducibility of the measurements was examined using 50 randomly selected participant scans, for which intra-reader variability was assessed by calculating the intraclass correlation coefficient (ICC) [26]. The ICCs for perirenal fat thickness were 0.984 (95% confidence interval [CI], 0.972 to 0.991; P<0.01) and 0.872 (95% CI, 0.785 to 0.925; P<0.01) for the left and right kidney, respectively. The total perirenal fat thickness was defined as the sum of perirenal fat thickness on both sides, and it was classified as Q1 (the lowest quartile) to Q4 (the highest quartile) in each sex, as males have more perirenal fat than females (Supplemental Table S1) [24].
Statistical analysis
Patients' clinical characteristics according to the quartiles of perirenal fat thickness were compared using analysis of variance or the Kruskal-Wallis test for continuous variables and the chi-square test for categorical variables. To investigate independent factors determining the presence of calcification, a binary logistic regression model was generated with adjustment for age, sex, hypertension, dyslipidemia, obesity, current smoking status, and family history of heart diseases in first-degree relatives. A receiver operating characteristic curve was used to evaluate the diagnostic performance of the detection of arterial bed calcification, and values of the area under the receiver operating characteristic curve (AUROC) were compared using the bootstrap method (n=1,000). P values <0.05 were considered to indicate statistical significance. All statistical analyses were conducted using SPSS version 24.0 (IBM Inc., Armonk, NY, USA) and the R 3.5.3. program (http://www.R-project.org; Vienna, Austria).
RESULTS
Clinical characteristics according to perirenal fat thickness on CT
The mean age of the sample was 56±11 years, and 55.6% were male (Table 1). The prevalence of arterial calcification was 53.3% in the coronary arteries, 26.2% in the carotid arteries, 34.8% in the thoracic aorta, 52.4% in the abdominal aorta, 47.1% in the iliac arteries, and 12.5% in the renal arteries (9.2% and 8.3% in the left and right renal arteries, respectively). Among all subjects with renal arterial calcification (n=488), 198 (40.6%) had calcification in both renal arteries, 126 (25.8%) in the right kidney only, and 164 (33.6%) in the left kidney only. The median total perirenal fat thickness was 13.0 cm (interquartile range [IQR], 8.1 to 18.4) and 5.3 cm (IQR, 3.4 to 8.1) in males and females, respectively (Supplemental Table S1). There was a strong correlation between right and left perirenal fat thickness (Spearman ρ=0.866; P<0.001).

Clinical Characteristics of the Study Subjects According to Perirenal Fat Thickness
Increasing perirenal fat thickness was associated with older age (mean age 50.4±10.3, 54.7±10.4, 57.4±10.7, and 60.6±10.2 years in Q1 to Q4, respectively; P<0.01) and more severe obesity (median BMI, 23.9 kg/m2 [IQR, 21.9 to 26.0], 26.0 kg/m2 [IQR, 23.5 to 28.0], 27.0 kg/m2 [IQR, 25.0 to 29.8], and 29.9 kg/m2 [IQR, 27.0 to 32.3], respectively; P<0.01). The prevalence of obesity, hypertension, and dyslipidemia also increased as perirenal fat thickness increased (P<0.01) (Table 1). In the crude analysis, a significant association was found between perirenal fat thickness quartiles and vascular calcification in each arterial bed (P<0.01 in all arterial beds) (Table 1).
Prevalence of arterial calcification according to perirenal fat thickness
In the crude analysis, as perirenal fat thickness increased by quartile, the odds of coronary and carotid calcification increased (odds ratio [OR], 1.386; 95% CI, 1.308 to 1.468; and OR, 1.520; 95% CI, 1.420 to 1.627, respectively) (Table 2). Calcification in the thoracic aorta, abdominal aorta, iliac arteries, and renal arteries also showed significant associations with perirenal fat thickness (Table 2). After adjustment for age, sex, BMI, hypertension, HDL-C, non-HDL-C, smoking history, and family history of heart disease in first-degree relatives, only vascular calcification in the coronary, carotid, and renal arteries were significantly associated with perirenal fat thickness (model 2 in Table 2). Specifically, renal arterial calcification was independently associated with perirenal fat in this model (OR per quartile of perirenal fat thickness, 1.251; 95% CI, 1.091 to 1.435) (model 2 in Table 2). Moreover, compared to Q1, the odds of renal arterial calcification increased along with perirenal fat thickness, with ORs of 1.399 (95% CI, 0.893 to 2.191; P=0.142), 1.786 (95% CI, 1.153 to 2.768; P=0.009), and 2.050 (95% CI, 1.294 to 3.250; P=0.002) for Q2 to 4, respectively (Table 2, Fig. 1A, Supplemental Table S2). Similarly, the ORs for carotid artery, thoracic aorta, and abdominal aorta calcification for each increase in the perirenal fat thickness quartile were modest, but significant: 1.118 (95% CI, 1.006 to 1.241; P=0.037), 1.141 (95% CI, 1.030 to 1.264; P=0.011), and 1.117 (95% CI, 1.013 to 1.23; P=0.027), respectively (Table 2, Fig. 1A).

Risk of Arterial Calcification According to Perirenal Fat Thickness (per Quartile)
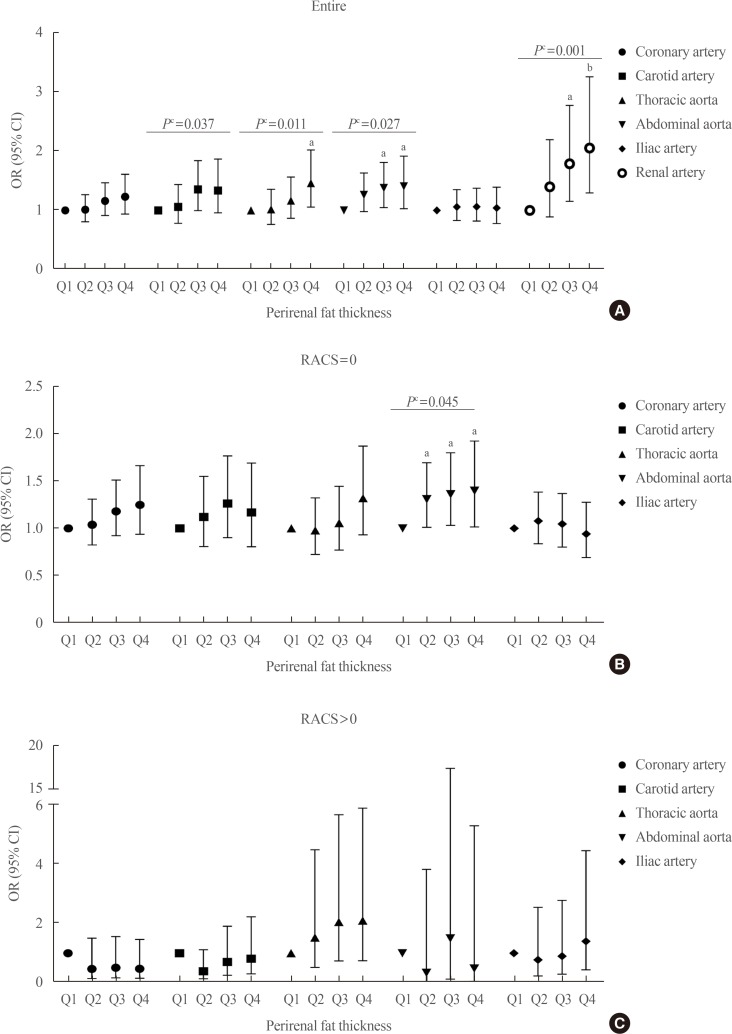
The risk of arterial calcification according to the quartiles of perirenal fat thickness. Total perirenal fat thickness was defined as the sum of perirenal fat thickness of both sides, and it was classified as Q1 (the lowest quartile) to Q4 (the highest quartile). Odds ratios (ORs) with 95% confidence interval (CIs) of the calcification in each arterial bed according to the perirenal fat thickness are shown (A) in the entire population, (B) those without renal artery calcification, and (C) in those with renal artery calcification. All statistical values were adjusted for age, sex, body mass index, hypertension, high-density lipoprotein cholesterol (HDL-C), non-HDL-C, smoking history, and family history of heart disease in first-degree relatives. RACS, renal artery calcification score. aP<0.05 compared to Q1; bP<0.005 compared to Q1; cP for trend.
A sensitivity analysis according to sex also confirmed the significance of the association between perirenal fat thickness and renal artery calcification in both sexes (Supplemental Table S3). A significant association between perirenal fat thickness and arterial calcification was not found in both sexes for any arterial bed other than the renal artery (Supplemental Table S3).
The risk of renal arterial calcification on each side was evaluated according to the ipsilateral and contralateral perirenal fat thickness. No location-specific differences in the association between renal arterial calcification and perirenal fat thickness were found (Supplemental Table S4), and the AUROC values for the prediction of renal arterial calcification by the ipsilateral and contralateral perirenal fat thickness were similar (Supplemental Table S5). The AUROC for the prediction of renal artery calcification using total perirenal fat was higher than the AUROCs obtained when using either the contralateral fat or ipsilateral fat, although there was no statistically significant difference. In females, the AUROC of right perirenal fat thickness for the prediction of left renal arterial calcification was significantly lower than that of total perirenal fat thickness (P=0.008); however, it was not significantly different from that of left perirenal fat thickness (P=0.452). Similarly, the AUROC of left perirenal fat thickness for the prediction of right renal arterial calcification was lower than that of total perirenal fat thickness (P=0.006) in females (Supplemental Table S5).
Calcification in different arterial beds according to the status of renal arterial calcification
Since renal arterial calcification itself is a well-known risk factor for both hypertension and systemic atherosclerosis [27], and because a strong association between renal fat thickness and renal arterial calcification was found in the current study (Fig. 1A), the association between perirenal fat thickness and vascular calcification in the other arterial beds was re-evaluated according to the presence or absence of renal arterial calcification (Fig. 1B, C). In subjects with renal arterial calcification, the prevalence of vascular calcification in each arterial bed reached >70% irrespective of perirenal fat thickness (Table 3). Even in Q1, the prevalence of vascular calcification in the coronary arteries, carotid arteries, thoracic aorta, and abdominal aorta was 83.0%, 70.7%, 74.5%, and 93.6%, respectively. No significant association was found between the prevalence of arterial calcification and perirenal fat thickness in those with renal arterial calcification after adjustment for confounders (Table 3).

Prevalence of Vascular Calcification According to Perirenal Fat Thickness
By contrast, in subjects without renal arterial calcification, a significant trend in the prevalence of arterial calcification according to perirenal fat thickness was found (P<0.001 for all in the crude analysis) (Table 3). Subsequent adjustment for age, sex, BMI, hypertension, HDL-C, non-HDL-C, smoking history, and family history of heart disease in first-degree relatives attenuated the statistical significance of these trends. Only abdominal aorta calcification remained significant (P for trend=0.045) (Table 3). For each 1-quartile increase in perirenal fat thickness, the odds of abdominal aorta calcification increased by 10% (OR, 1.109; 95% CI, 1.003 to 1.228; P=0.045) (model 2 in Table 4). The ORs for abdominal aorta calcification in Q2, Q3, and Q4 compared to Q1 were 1.305 (95% CI, 1.010 to 1.305; P=0.042), 1.357 (95% CI, 1.029 to 1.791; P=0.031), and 1.393 (95% CI, 1.013 to 1.916; P=0.041), respectively (Fig. 1B).

Risk of Arterial Calcification According to Perirenal Fat Thickness (per Quartile) in Subjects without Renal Artery Calcification
DISCUSSION
The results of the current study suggest that perirenal fat thickness is significantly associated with the presence of renal arterial calcification. Even after adjustment for atherosclerotic risk factors such as age, obesity, dyslipidemia, hypertension, smoking history, and family history, the risk of renal arterial calcification increased by 25% with every quartile of perirenal fat thickness. Perirenal fat thickness was also associated with calcified atherosclerosis in the other vascular beds evaluated (the carotid arteries, coronary arteries, thoracic aorta, abdominal aorta, iliac arteries, and renal arteries); however, after adjustment for renal arterial calcification and atherosclerotic risk factors, it was only associated with abdominal aorta calcification.
Perirenal fat is, like other ectopic fat, an active secretory organ that produces adipokines and cytokines [2829], which induce inflammation [678], and consequently, atherosclerosis [18910]. The current findings that perirenal fat thickness was significantly associated not only with dyslipidemia or hypertension, but also with systemic arterial calcification, and that the significant association between vascular calcification and perirenal fat thickness was attenuated by adjustment for atherosclerotic risk factors, suggest a systemic effect of perirenal fat on the atherosclerotic process. Nevertheless, the presence of an independent association between renal artery calcification and perirenal fat thickness in a dose-dependent manner suggests that perirenal fat exerts a local effect on the renal arteries. Furthermore, in females, the prediction of renal artery calcification by contralateral perirenal fat thickness was less powerful than the use of total perirenal fat thickness. Perirenal fat is known to induce a local inflammatory response [30] and to regulate renal physiology [3031]. Nonetheless, no significant difference was found in the effect of perirenal fat thickness between the ipsilateral and contralateral renal arteries in the current study. The AUROC for the prediction of renal artery calcification using total perirenal fat was higher than the AUROC values obtained for both the contralateral fat and ipsilateral fat, even though the difference did not reach statistical significance. We could not differentiate fat inside the renal fascia from the fat outside the fascia, which may have attenuated the local effects of perirenal fat. Considering that renal sinus fat increases renal hydrostatic pressure and activates the renin-angiotensin-aldosterone system [1516], fat inside the renal fascia might have a more direct effect on the renal arteries than perirenal fat outside the fascia. In addition, in the current study, both perirenal fat thickness and renal arterial calcification on both sides were strongly correlated with each other, which might have caused the absence of a difference between the ipsilateral and contralateral associations. Further studies to determine the local effects of perirenal fat are needed.
Renal arterial calcification is an independent risk factor for all-cause mortality even in healthy outpatients without any cardiovascular disease [27]. A stratified analysis according to the presence of renal arterial calcification in the current study confirmed that the presence of renal artery calcification reflects a high risk of systemic atherosclerosis. Specifically, the prevalence of vascular calcification in the other arterial beds among those with renal artery calcification was more than 70% in each arterial bed, irrespective of the amount of perirenal fat. By contrast, in those without renal arterial calcification, a significant trend in the prevalence of arterial calcification according to perirenal fat thickness was found in all arterial beds in the crude analysis, which implies that the effects of ectopic fat such as perirenal fat might be different according to the severity of the systemic atherosclerosis burden, and that reduction of ectopic fat might have a more favorable effect on cardiometabolic health in the early stages of atherosclerosis.
Interestingly, in those without renal arterial calcification, the only independent association between vascular calcification and perirenal fat thickness was found for abdominal aorta calcification, although its OR per quartile was around 1.2. Currently, it is not apparent why perirenal fat thickness was independently associated with calcification in the abdominal aorta, but not in the other vascular beds. The prevalence of calcification in abdominal aorta and coronary arteries was relatively high compared to the other arteries in the current study, which might have strengthened the statistical significance of this finding despite the similar ORs. In addition, the relatively short anatomical distance between perirenal fat and the abdominal aorta might have contributed to this finding, and this possibility should be explored in another independent study.
A limited number of studies have estimated perirenal fat thickness using CT scans [1724]. In most previous studies, perirenal fat thickness was assessed using ultrasonography [121314]. Although ultrasonography is more convenient, CT scans enable a full-scale measurement [32]. In addition, perirenal fat thickness assessed by CT scans was reported to be a reliable marker of perirenal fat volume [17].
The current study has several limitations. First, as mentioned above, we did not differentiate fat inside the renal fascia from the fat outside the fascia, which might have masked the local effects of perirenal fat. Few studies have compared the effects of fat on both sides. Although both pararenal fat [13] as well as renal sinus fat [3334] have been reported to be independent risk factors for hypertension even after adjustment for visceral fat, the fat inside the renal fascia might exert a more direct effect on the renal arteries than the perirenal fat outside the fascia via the renin-angiotensin-aldosterone system [1516] and local inflammation [8]. Second, we did not measure waist circumference or intra-abdominal visceral fat, although a comparison of the effect of perirenal fat to that of other visceral fat on systemic atherosclerotic calcification would enable the pathophysiological role of perirenal fat distinct from other visceral fat to be elucidated. In addition, no information on fasting lipid levels was analyzed in the current study. However, the ratio of total to HDL-C [3536] and non-HDL-C [37] used in the current study has been reported to be a good predictor of future cardiovascular diseases. Lastly, the cross-sectional nature of the study makes it impossible to identify the causal relationships underlying the association between perirenal fat and arterial calcification.
A major strength of the study is that the current findings are based on a large community-based cohort that underwent extensive evaluations of systemic calcification, including six arterial beds in each of 3,919 subjects. Furthermore, few previous studies have investigated the association between perirenal fat thickness and systemic atherosclerotic calcification.
In the current study, we confirmed that perirenal fat thickness was independently associated with vascular calcification in the renal artery and abdominal aorta. Further epidemiological studies to replicate the current findings are needed in diverse study populations.
ACKNOWLEDGMENTS
This study was supported by the National Institute of Health (Ro 1 DK080015).
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS:
Conception or design: B.K.K., M.A.A.
Acquisition, analysis, or interpretation of data: B.K.K., J.O.D., C.M.W., M.H.C., M.A.A.
Drafting the work or revising: B.K.K., C.M.W., M.H.C., M.A.A.
Final approval of the manuscript: B.K.K., J.O.D., C.M.W., M.H.C., M.A.A.
References
SUPPLEMENTARY MATERIALS
Supplemental Table S1
Body Mass Index and Perirenal Fat Thickness by Sex
Supplemental Table S2
Odds of Arterial Calcification in Each Perirenal Fat Thickness Quartile (Q2–4) Compared to the Lowest Quartile (Q1)
Supplemental Table S3
Risk of Arterial Calcification According to Perirenal Fat Thickness (per Quartile) in Each Sex
Supplemental Table S4
Risk of Renal Arterial Calcification According to Perirenal Fat Thickness (per Quartile)
Supplemental Table S5
Prediction of the Presence of Renal Arterial Calcification by Perirenal Fat Thickness
Supplemental Fig. S1
Measurement of perirenal fat thickness. Computed tomography evaluation of perirenal fat thickness was the distance from kidney to nearest viscera or muscle, and five perirenal measurements were taken: lateral (A), posterolateral (B), posterior (C), anterolateral (D), and medial (E) on a slice passing through the renal vein.



