An Unusual Case of Meningioma Showing Increased CaSR Expression with Parathyroid Carcinoma
Article information

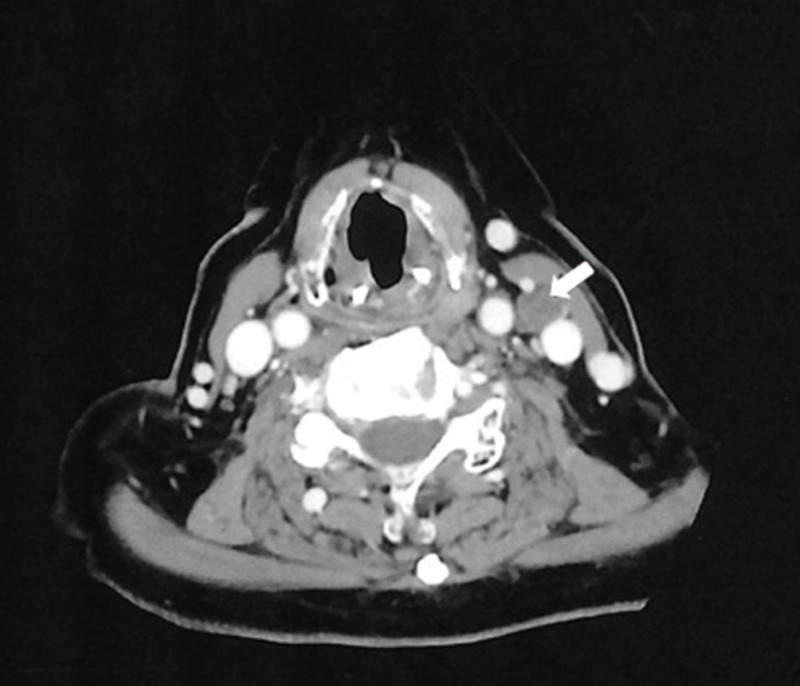
A 68-year-old woman with a history of parathyroidectomy of the left upper and right lower parathyroid gland for parathyroid carcinoma was admitted to our hospital for evaluation of fatigue and anorexia that lasted for 1 month. Blood chemistry was notable for hypercalcemia (14.1 mg/dL) and elevated parathyroid hormone (PTH) 1,652 pg/mL (0.35 to 5.50). Serum PTH-related peptide (PTHrP) level was measured at 33.2 pmol/L (13.8 to 55.3). T-score of spine and femur neck measured by dual energy X-ray absorptiometry was −3.12 and −4.15, suggesting osteoporosis. Computed tomography scan of the neck found a nodule sized 1×1.2 cm on the left neck (Fig. 1) [1]. She developed two episodes of myoclonic seizures at the 9th day on hospitalization. Magnetic resonance imaging of the brain found a 3×4 cm sized lesion on her left frontal lobe later reported as meningioma (Fig. 2A) [1]. Surgical resection of the meningioma and the left cervical mass was performed. Pathology of the cervical mass found hyperplasia of parathyroid gland, suggesting recurrence of parathyroid carcinoma. Thirteen years after the diagnosis of meningioma, we performed immunohistochemistry on the meningeal tissue for calcium-sensing receptor (CaSR) at the meninges and found strong CaSR expression (Fig. 2B).
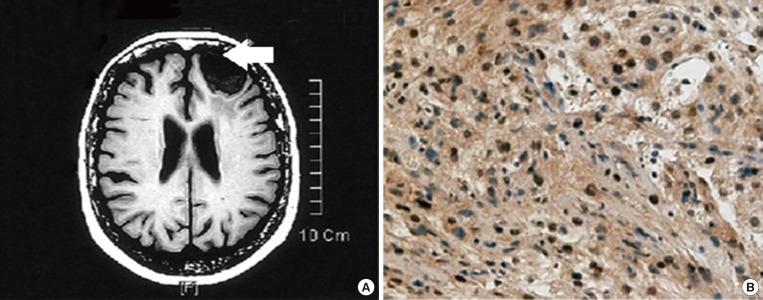
(A) Magnetic resonance imaging of the meningioma. A 3×4 cm sized extra-axial tumor along the left frontal convexity consistent with meningioma is noted (arrow). Adapted from Ju et al. [1]. (B) Immunohistochemical localization of calcium sensing receptor (CaSR) in meningioma. Strong CaSR-antibody (diluted 1:500, Novus Biologicals) reactivity in meningioma tissue is notable (×200).
It has been known that CaSR has oncogenic properties and over-expression of CaSR is observed in some metastasizing breast, prostate cancer, and meningioma [23]. Enhanced CaSR expression on meningeal cells and elevated calcium level due to parathyroid carcinoma would be a trigger for meningioma [4]. Enhanced PTHrP expression has also known to be observed in meningioma [45]; however, in this case PTHrP concentration in blood was within normal range. Additionally, the coincidence of parathyroid carcinoma and meningioma may infer the presence of multiple endocrine neoplasia type 1 (MEN1) cancer syndrome, whose diagnosis needs DNA testing [6].
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.