
Articles
- Page Path
- HOME > Endocrinol Metab > Volume 28(1); 2013 > Article
-
Original ArticleThe Relationship of Body Composition and Coronary Artery Calcification in Apparently Healthy Korean Adults
- Jung-Hee Yu, Seo Hyoung Yim, Su Hyeon Yu, Ji Yong Lee, Jong Dae Kim, Mi Hae Seo, Won Seon Jeon, Se-Eun Park, Cheol-Young Park, Won-Young Lee, Ki-Won Oh, Sung-Woo Park, Eun-Jung Rhee
-
Endocrinology and Metabolism 2013;28(1):33-40.
DOI: https://doi.org/10.3803/EnM.2013.28.1.33
Published online: March 25, 2013
Division of Endocrinology, Department of Internal Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea.
- Corresponding author: Eun-Jung Rhee. Division of Endocrinology, Department of Internal Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, 29 Saemunan-ro, Jongno-gu, Seoul 110-746, Korea. Tel: +82-2-2001-2485, Fax: +82-2-2001-1588, hongsiri@hanmail.net
Copyright © 2013 Korean Endocrine Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,871 Views
- 29 Download
- 24 Crossref
ABSTRACT
-
Background
- We investigated the association of coronary artery calcium score (CACS) with body composition and insulin resistance in apparently healthy Korean adults.
-
Methods
- Nine hundred forty-five participants (mean age, 48.9 years; 628 men) in a medical check-up program were selected for analysis. Body composition was assessed by bioelectrical impedance analysis (BIA). Insulin resistance was evaluated using the homeostasis model assessment of insulin resistance (HOMA-IR). The CACS was assessed by multidetector computed tomography.
-
Results
- One hundred forty-six subjects (15.4%) showed coronary artery calcification and 148 subjects (15.7%) had metabolic syndrome. CACS showed a significant positive correlation with age, fasting glucose level, waist circumference (WC), blood pressure, hemoglobin A1c, HOMA-IR, and waist-hip ratio (WHR) assessed by BIA. CACS had a negative correlation with high density lipoprotein cholesterol (HDL-C). Subjects with high CACS showed significantly higher mean WHRs and lower mean values for lean body mass compared with subjects without coronary artery calcification. In logistic regression analyses with coronary artery calcification as the dependent variable, the highest quartile of WHR showed a 3.125-fold increased odds ratio for coronary artery calcification compared with the lowest quartile after adjustment for confounding variables. When receiver operating characteristics analyses were performed with coronary artery calcification as the result variable, WHR showed the largest area under the curve (AUC) value among other variables except for age and WC in women (AUC=0.696 for WHR, 0.790 for age, and 0.719 for WC in women).
-
Conclusion
- In our study population of apparently healthy Korean adults, WHR was the most significant predictor for coronary artery calcification among other confounding factors, suggesting that it may have implication as a marker for early atherosclerosis.
- Adipose tissue is not simply a mass of fat, but an active endocrine organ that modifies the metabolic status of the human body [1]. Recent studies emphasize the importance of depots where fat is accumulated rather than the simple fat mass, and visceral obesity is known to be a strong risk factor for metabolic and subsequent cardiovascular disease (CVD) [2].
- Early detection of subclinical atherosclerosis is important to prevent overt atherosclerosis [3]. Coronary artery calcium score (CACS) is a risk marker for atherosclerosis and is positively associated with CVD events [4]. The development of multislice computed tomography enabled the reliable detection and quantification of CAC that correlates with the overall atherosclerotic plaque burden [5]. There are studies reporting that visceral adiposity and insulin resistance are significant risk factors for the development of subclinical atherosclerosis, as assessed by CACS, in apparently healthy subjects without previous history of CVD [6-9]. In addition, a few studies have reported an association between body composition and the development of metabolic and CVDs [10,11]. The importance of strategies to lessen abdominal adiposity, modify the body composition, and improve insulin resistance would be of great benefit to prevent atherosclerosis even in healthy subjects without documented CVD.
- The aim of this study was to analyze the relationship between body composition assessed by bioelectric impedance analysis (BIA) and coronary artery calcification assessed by multidetector computed tomography (MDCT) in asymptomatic healthy Korean adults.
INTRODUCTION
- Study participants
- Among the subjects who participated in the medical check-up program at Kangbuk Samsung Hospital's Health Promotion Center from 2007 through 2009, 945 subjects (mean age, 48.9 years; range, 28 to 82 years; 628 men, 66.5%) with CACS data were selected for analysis. The study protocol conforms to ethical guidelines of the 1975 Declaration of Helsinki, and accordingly the Kangbuk Samsung Hospital Human Research Committee approved it. The informed consent requirement for this study was deemed exempt by the Institutional Review Board at the time the study was in the planning phase because researchers only accessed the database, which was free of identifying personal information, for analysis purposes.
- Clinical and laboratory measurement
- Height, weight, systolic and diastolic blood pressures were measured in duplicate and the results were averaged. The blood pressures were taken with a standardized sphygmomanometer after at least 5 minutes of rest, according to the Hypertension Detection and Follow-up Program protocol [12]. The body mass index (BMI) was calculated by dividing the patient's weight (kg) by the height (m) squared. The waist circumference (WC) was measured in the standing position, at the midpoint between the anterior iliac crest and lower border of the last palpable rib by a single examiner.
- After 12 hours of fasting, fasting blood glucose, total cholesterol, triglyceride, high density lipoprotein cholesterol (HDL-C), and low density lipoprotein cholesterol (LDL-C) levels were checked. The hexokinase method (Advia 1650 Autoanalyzer, Bayer Diagnostics, Leverkusen, Germany) was used to measure blood glucose levels and an enzymatic colorimetric test was used to measure total cholesterol and triglyceride levels. The selective inhibition method was used to measure the level of HDL-C and a homogeneous enzymatic calorimetric test was used to measure the level of LDL-C. Serum insulin concentrations were measured with an immunoradiometric assay (INS-Irma, Biosource, Nivelles, Belgium), with intra and interassay coefficients of variation of 1.6% to 2.2% and 6.1% to 6.5%, respectively.
- Hemoglobin A1c (HbA1c) was measured by immunoturbidimetric assay with a Cobra Integra 800 automatic analyzer (Roche Diagnostics, Basel, Switzerland) with a reference value of 4.4% to 6.4%. The methodology was aligned with the Diabetes Control and Complications Trial and National Glycohemoglobin Standardization Program (NGSP) standards [13]. The intra-assay coefficient of variation (CV) was 2.3% and interassay CV was 2.4%, both within the NGSP acceptable limits [14]. The glycemic statuses of the participants were determined according to the self-questionnaire of the participants and the American Diabetes Association's diagnostic criteria [15].
- Assessment of insulin resistance was calculated by homeostasis model assessment of insulin resistance (HOMA-IR) [16]: HOMA-IR=fasting insulin (µU/mL)×fasting glucose (mmol/L)/22.5.
- Body composition analyses by bioelectrical impedance analyses
- Body composition measurements were carried out by segmental bioelectric impedance, using eight tractile electrodes according to the manufacturer's instructions (InBody 3.0, Biospace, Seoul, Korea). Lean mass (kg), fat mass (kg), percent fat mass (%), and waist-hip ratio (WHR) as a marker of abdominal obesity, were measured.
- Measurement of CACS
- The CAC imaging was performed using MDCT (Philips Brilliance 40 slice, Amsterdam, The Netherlands). The 40-slice MDCT was performed using the following protocol: 0.625 mm slice thickness, 120 kVp, 800 effective mAs, and a 0.4-second gantry rotation speed. CACS were expressed in Agatston units and CACS [17] as significant or CAC positive status. Having coronary artery calcification was defined as having CACS>0.
- Subjects were divided into three groups according to CACS; group with CACS=0, 1<CACS<100, and CACS≥100. The reason for dividing the subjects into three groups instead or four or five groups as with previous studies [17], was because there were too few subjects with CACS higher than 1 (n=146, 15.4%).
- Statistical analyses
- All data are presented as the mean and standard deviation, and were analyzed using IBM SPSS version 18.0 for Windows (IBM, Armonk, NY, USA). Bivariate correlation analyses between coronary calcium score and the other variables were performed using Pearson's correlation analysis. Comparison of the parameters among three groups divided by CACS was analyzed by one-way analysis of variance, and post-hoc analyses were performed with Tukey's method. Multiple logistic regression analyses were performed with coronary calcification as the dependent variable with other confounding variables included in the model. The variables included in the model were selected according to the results of bivariate correlation analyses. Receiver operating characteristics (ROC) curve analyses were performed to calculate the area under the curve (AUC) and the cutoff of each variable for coronary artery calcification. A P value <0.05 was considered statistically significant.
METHODS
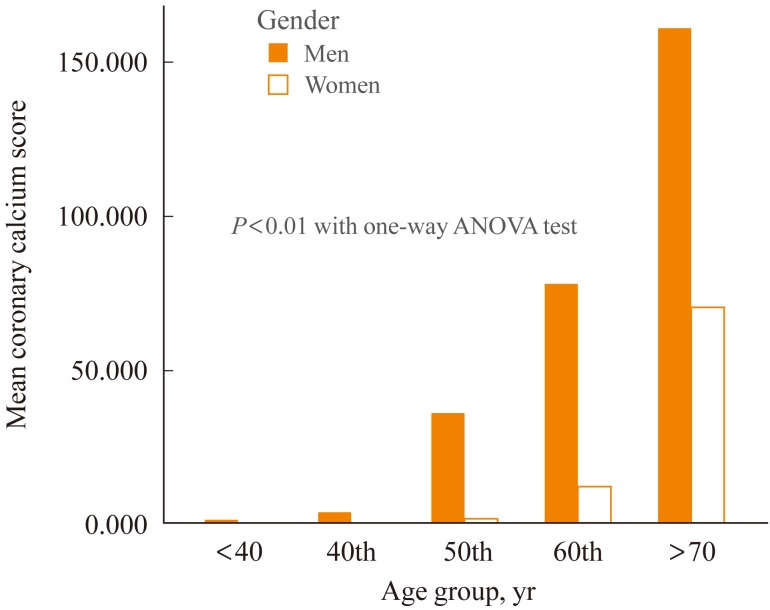
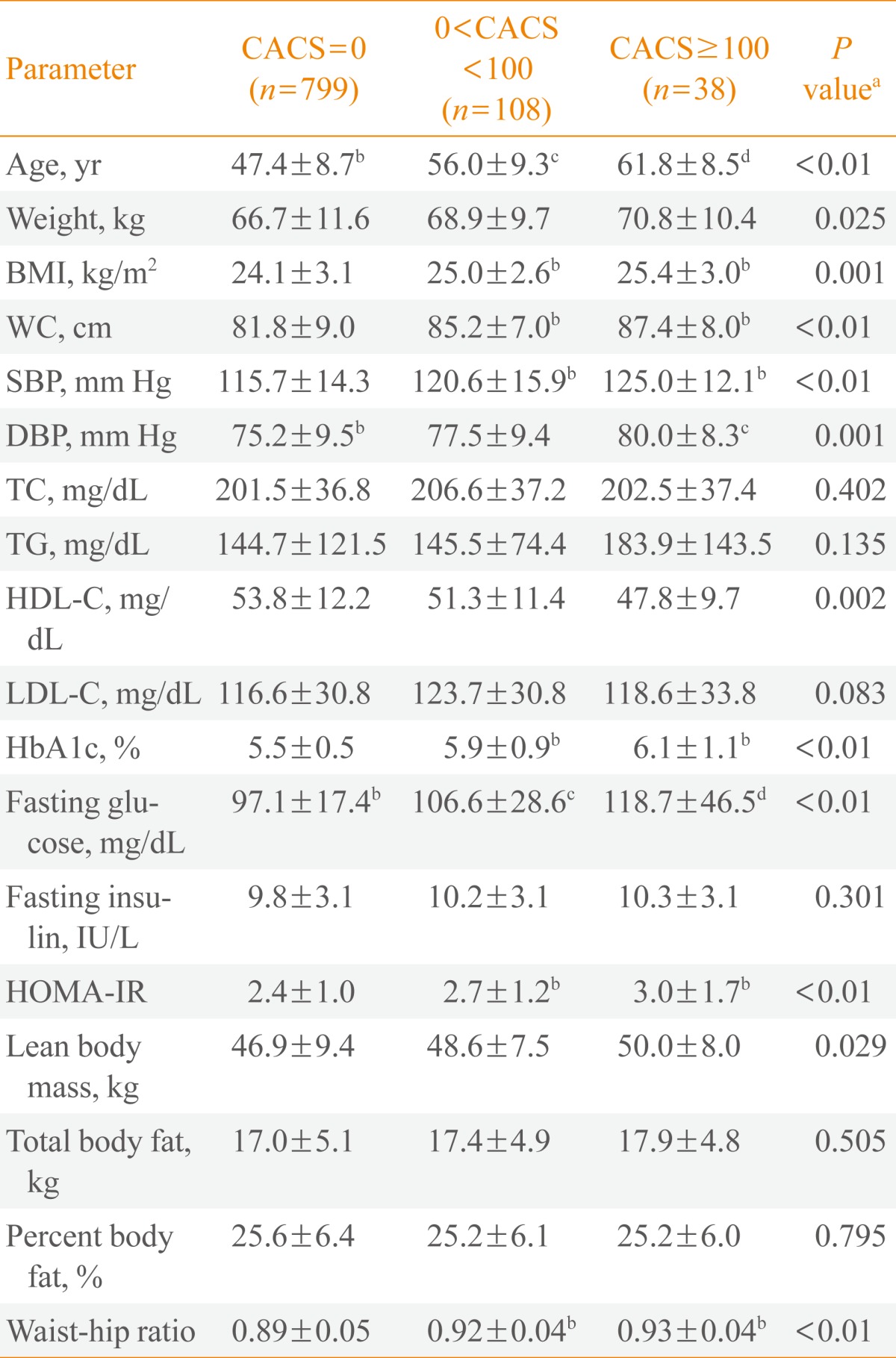
- Baseline characteristics of the participants are listed in Table 1. Mean age of the study sample was 48.9 years; 66.5% were men. One hundred forty-six subjects (15.4%) showed significant coronary artery calcification with a CACS greater than 0. Seven hundred ninety-nine subjects (84.6%) were normal, 108 subjects (11.4%) had a CACS less than 100, and 38 subjects (4.0%) had a CACS larger than or equal to 100 (Table 1). As the subjects got older, the mean CACS linearly increased (Supplemental Table S1 online, Fig. 1). Six hundred and fourteen subjects (65%) showed normoglycemia, 274 subjects (29.0%) showed impaired fasting glucose, and 57 subjects (6.0%) had diabetes. Men were more obese than women, but showed a higher lean body mass and less body fat compared with women. Women showed a lower prevalence for coronary artery calcification compared with men (Table 1).
- In bivariate correlation analysis, CACS showed a significant positive correlation with age, WC, blood pressure, HbA1c, fasting blood sugar (FBS), HOMA-IR, and WHR, and a negative correlation with HDL-C (Table 2). In women, CACS also showed a positive correlation with body fat mass.
- When the subjects were divided into three groups according to the CACS, subjects were older as the mean CACS increased from 0 to greater than 100 (Table 2). Mean values for body weight, BMI, WC, blood pressure, HbA1c, FBS, HOMA-IR, and WHR became higher and mean values for HDL-C became lower as the mean CACS increased from 0 to that greater than 100 (Table 3). In all groups, the mean value for lean body mass became lower as the mean CACS increased from 0 to that greater than 100; however, when the analysis was performed only in men, the mean value for lean body mass was significantly lower in subjects with a CACS higher than 0 and lower than 100 compared with subjects without coronary artery calcification (Supplemental Table S2 online). In women, mean lean body mass did not show any significant differences among the three groups (Supplemental Table S3 online). In contrast, for total body fat and percent body fat, subjects with coronary artery calcification showed significantly increased mean values as the CACS increased. Men did not show any differences among the three groups regarding total fat mass or percent body fat (Supplemental Table S2 online). Mean WHR significantly increased as the CACS increased from 0 to greater than 100 even when the analyses were performed separately for different genders (Supplemental Tables S2, S3 online).
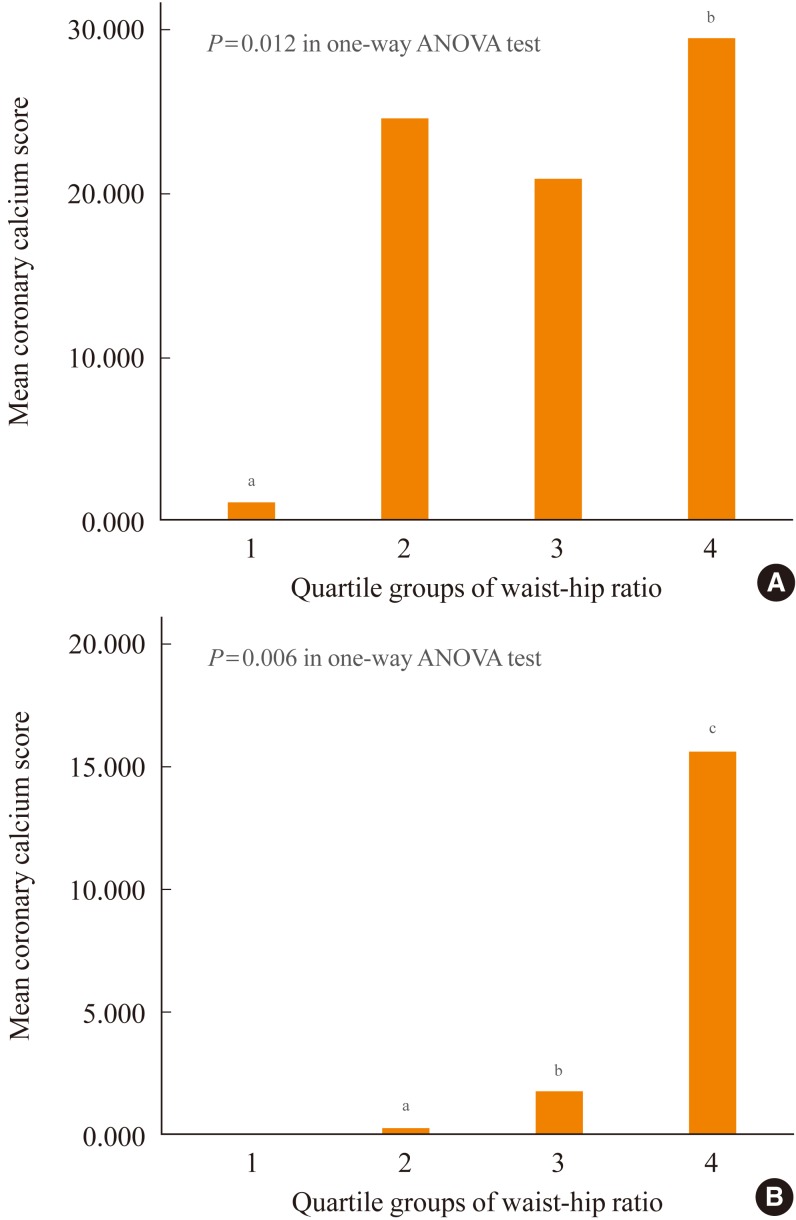
- When the subjects were divided into four groups according to WHR, mean CACS was significantly higher in the 4th quartile group compared to the 1st group in men (Supplemental Table S4 online, Fig. 2A). In women, mean values of CACS increased linearly from 1st to 4th quartile groups with significant differences between that of 1st quartile group and those of the other three quartile groups in post-hoc analyses (Supplemental Table S4 online, Fig. 2B).
- In logistic regression analyses with coronary artery calcification as the dependent variable, the 4th quartile group of WHR showed a 3.125-fold increased risk for coronary artery calcification compared to the lowest quartile group after adjustment for other confounding variables (Table 4). When ROC curve analyses were performed with coronary artery calcification as the result variable, WHR showed the largest AUC value among other variables except for age and WC in women (AUC=0.696 for WHR, 0.790 for age and 0.719 for WC in women) (Table 5).
RESULTS
- In this study, abdominal obesity assessed by WHR showed a significant positive correlation with CACS. The subjects with high CACS showed significantly worse metabolic parameters compared with those with low CACS, supporting the role of metabolic parameters in the development of subclinical atherosclerosis. In men, mean lean mass was significantly higher in subjects without coronary artery calcification compared to those with significant coronary artery calcification. In contrast, women showed a significant positive correlation between CACS and fat mass. In both genders, higher WHR showed an increased risk for coronary artery calcification, and WHR showed the highest AUC for the prediction of coronary calcification except for age and WC in women, suggesting that WHR plays a significant role as a marker for early atherosclerosis. This is the first study performed in Koreans regarding the relationship between body composition and coronary artery calcification.
- In this study, abdominal obesity assessed by WHR showed the most significant correlation with coronary artery calcification among the measured components of body composition analysis. This is in line with the result of a previous study [11]. The Dallas Heart Study analyzed the relationship between CACS and differing methods of measuring obesity in 2,744 multi-ethnic adults. They discovered that WHR was independently associated with prevalent coronary artery calcification and that WHR was a more accurate predictor than either BMI or WC. In the Jackson Heart Study performed in 2,884 subjects who underwent noncontrast CT, visceral adipose tissue was positively associated with CAC, but this association was diminished with multivariable adjustment [8]. Additionally, in a study performed in 321 Japanese subjects, Ohashi et al. [7] showed that visceral adiposity was significantly associated with CAC as a marker of subclinical atherosclerosis. From these previous studies and the results of our study, we can conclude that abdominal adiposity, especially assessed by WHR rather than overall fat mass, contributes more to the development of subclinical atherosclerosis in apparently healthy adults.
- The mechanistic reason for the association of visceral fat with atherosclerosis is explained fully in the previous literature. Although obesity as defined by BMI is undoubtedly associated with an increased cardiovascular risk, recent studies have emphasized on the metabolic differences between different types of obese subjects. For example, there are suggestions for a subset of obese subjects who are obese but metabolically healthy [18]. The main differences between the "metabolically healthy obese" and "metabolically unhealthy obese" subjects are in their fat depots. "Metabolically healthy obese" subjects have BMI levels similar to their metabolically unhealthy peers, but they tend to accumulate fat less in the abdomen, and more subcutaneously [19]. Therefore, in a sense, abdominal obesity in the absence of increased BMI, could negatively affect metabolic status and thus, vascular health. There is already strong consensus on the deleterious effects of visceral fat accumulation on the development of subclinical atherosclerosis and subsequently increased CVD risk [2].
- In this study, the effect of body composition on CACS was different between genders. Male subjects showed a negative correlation between lean body mass and coronary artery calcification, and women showed a positive correlation between body fat mass and coronary artery calcification. In the study by Alexandersen et al. [10], peripheral lean mass showed a strong and independent inverse association with aortic calcification assessed by lateral radiograph. Although the significant association of sarcopenia with CVD is not clear yet, recent studies strongly suggest the possible role of lack of muscle mass in the development of metabolic diseases [20]. The reason for the different correlation of CACS with different components of body composition between genders might be due to the role of sex hormones. In addition, since most of the female participants in this study were premenopausal, the degree of atherosclerosis might be very low, reflected in the significantly lower mean CACS in women compared with men. Also, the vasculoprotective effects of estrogen might still be present in these women, suggesting the level of estrogen might correlate with subclinical atherosclerosis, which is significantly correlated with body fat mass. This could explain why the positive correlation of CACS with fat mass was observed only in women.
- This study has several limitations. First, the study population was not representative of the Korean population. Therefore, the results of our study cannot be extrapolated to whole Korean population. Second, specific history of the participants such as smoking, past medical history and medication were not available for analysis. Third, since this was a cross-sectional study, a cause-and-effect relationship cannot be determined from the study. Lastly, the BIA method used for the measurement of body composition analyses was not as accurate as dual X-ray absorptiometry; thus the assessment of specific components of body composition could have had some biases and limitations. In spite of these limitations, this study is meaningful in that it is the first study performed in Koreans regarding the relationship between body composition and CACS.
- In conclusion, we found that WHR showed a significantly higher correlation with coronary artery calcification compared with other metabolic parameters in Korean adults. This result suggests the superiority of WHR as the marker for early atherosclerosis compared to other parameters that assess obesity status. In addition, our study adds to the body of knowledge suggesting that abdominal obesity may have significant deleterious effects, particularly the development of atherosclerosis with the potential for future cardiovascular risk. Further, prospective studies are needed to determine whether WHR is associated with presence of CAC across different ethnic groups in apparently healthy subjects.
DISCUSSION
-
Acknowledgements
- This work was supported by grant from Sungkyunkwan University Industry-Academy Cooperation Group.
ACKNOWLEDGMENT
Supplementary Material
- 1. Fortuno A, Rodriguez A, Gomez-Ambrosi J, Fruhbeck G, Diez J. Adipose tissue as an endocrine organ: role of leptin and adiponectin in the pathogenesis of cardiovascular diseases. J Physiol Biochem 2003;59:51–60. ArticlePubMedPDF
- 2. Mathieu P, Pibarot P, Larose E, Poirier P, Marette A, Despres JP. Visceral obesity and the heart. Int J Biochem Cell Biol 2008;40:821–836. ArticlePubMed
- 3. Simon A, Levenson J. May subclinical arterial disease help to better detect and treat high-risk asymptomatic individuals? J Hypertens 2005;23:1939–1945. ArticlePubMed
- 4. Greenland P, LaBree L, Azen SP, Doherty TM, Detrano RC. Coronary artery calcium score combined with Framingham score for risk prediction in asymptomatic individuals. JAMA 2004;291:210–215. ArticlePubMed
- 5. Nasir K, Clouse M. Role of nonenhanced multidetector CT coronary artery calcium testing in asymptomatic and symptomatic individuals. Radiology 2012;264:637–649. ArticlePubMed
- 6. Lee CD, Jacobs DR Jr, Schreiner PJ, Iribarren C, Hankinson A. Abdominal obesity and coronary artery calcification in young adults: the Coronary Artery Risk Development in Young Adults (CARDIA) Study. Am J Clin Nutr 2007;86:48–54. ArticlePubMedPDF
- 7. Ohashi N, Yamamoto H, Horiguchi J, Kitagawa T, Hirai N, Ito K, Kohno N. Visceral fat accumulation as a predictor of coronary artery calcium as assessed by multislice computed tomography in Japanese patients. Atherosclerosis 2009;202:192–199. ArticlePubMed
- 8. Liu J, Musani SK, Bidulescu A, Carr JJ, Wilson JG, Taylor HA, Fox CS. Fatty liver, abdominal adipose tissue and atherosclerotic calcification in African Americans: the Jackson Heart Study. Atherosclerosis 2012;224:521–525. ArticlePubMedPMC
- 9. Arad Y, Newstein D, Cadet F, Roth M, Guerci AD. Association of multiple risk factors and insulin resistance with increased prevalence of asymptomatic coronary artery disease by an electron-beam computed tomographic study. Arterioscler Thromb Vasc Biol 2001;21:2051–2058. ArticlePubMed
- 10. Alexandersen P, Tanko LB, Bagger YZ, Jespersen J, Skouby SO, Christiansen C. Associations between aortic calcification and components of body composition in elderly men. Obesity (Silver Spring) 2006;14:1571–1578. ArticlePubMed
- 11. See R, Abdullah SM, McGuire DK, Khera A, Patel MJ, Lindsey JB, Grundy SM, de Lemos JA. The association of differing measures of overweight and obesity with prevalent atherosclerosis: the Dallas Heart Study. J Am Coll Cardiol 2007;50:752–759. ArticlePubMed
- 12. Curb JD, Ford C, Hawkins CM, Smith EO, Zimbaldi N, Carter B, Cooper C. A coordinating center in a clinical trial: the Hypertension Detection and Followup Program. Control Clin Trials 1983;4:171–186. ArticlePubMed
- 13. NGSP. List of NGSP certified methods [Internet]; [place unkown]: NSGP; c2010. updated 2013 Feb 1. cited 2012 Nov 26. Available from: http://www.ngsp.org/docs/methods.pdf.
- 14. Schwartz KL, Monsur JC, Bartoces MG, West PA, Neale AV. Correlation of same-visit HbA1c test with laboratory-based measurements: a MetroNet study. BMC Fam Pract 2005;6:28ArticlePubMedPMCPDF
- 15. American Diabetes Association. Standards of medical care in diabetes: 2011. Diabetes Care 2011;34(Suppl 1):S11–S61. ArticlePubMedPMC
- 16. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985;28:412–419. ArticlePubMedPDF
- 17. Rumberger JA, Brundage BH, Rader DJ, Kondos G. Electron beam computed tomographic coronary calcium scanning: a review and guidelines for use in asymptomatic persons. Mayo Clin Proc 1999;74:243–252. ArticlePubMed
- 18. Bluher M. Are there still healthy obese patients? Curr Opin Endocrinol Diabetes Obes 2012;19:341–346. ArticlePubMed
- 19. Samocha-Bonet D, Chisholm DJ, Tonks K, Campbell LV, Greenfield JR. Insulin-sensitive obesity in humans: a 'favorable fat' phenotype? Trends Endocrinol Metab 2012;23:116–124. ArticlePubMed
- 20. Kim TN, Park MS, Lim KI, Yang SJ, Yoo HJ, Kang HJ, Song W, Seo JA, Kim SG, Kim NH, Baik SH, Choi DS, Choi KM. Skeletal muscle mass to visceral fat area ratio is associated with metabolic syndrome and arterial stiffness: the Korean Sarcopenic Obesity Study (KSOS). Diabetes Res Clin Pract 2011;93:285–291. ArticlePubMed
References
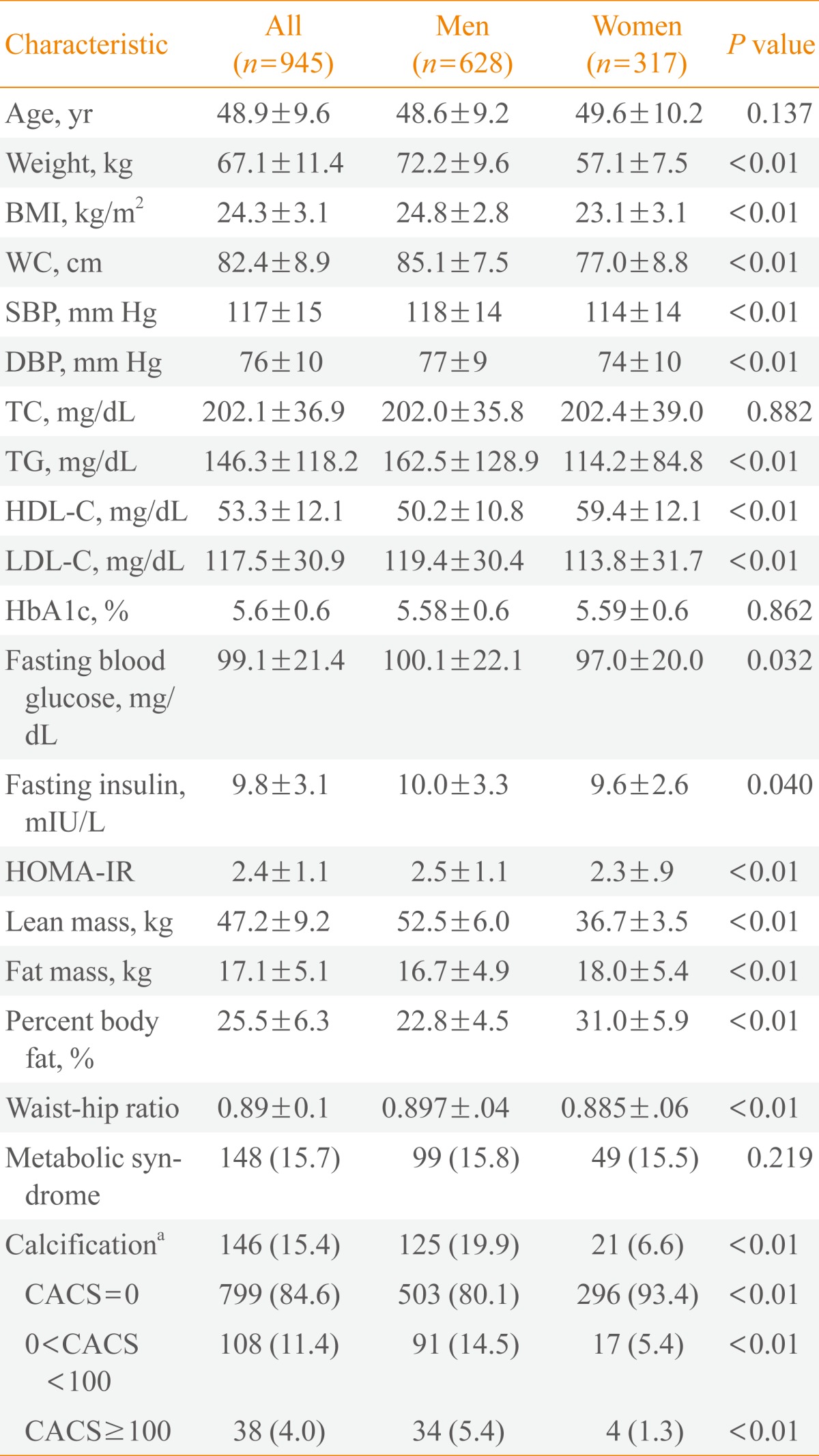
Values are expressed as mean±SD or number (%).
BMI, body mass index; WC, waist circumference; SBP, systolic blood pressure; DBP, diastolic blood pressure; TC, total cholesterol; TG, triglyceride; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; HbA1c, hemoglobin A1c; HOMA-IR, homeostasis model assessment of insulin resistance; CACS, coronary artery calcium score.
aHaving coronary artery calcification was defined by CACS>0.
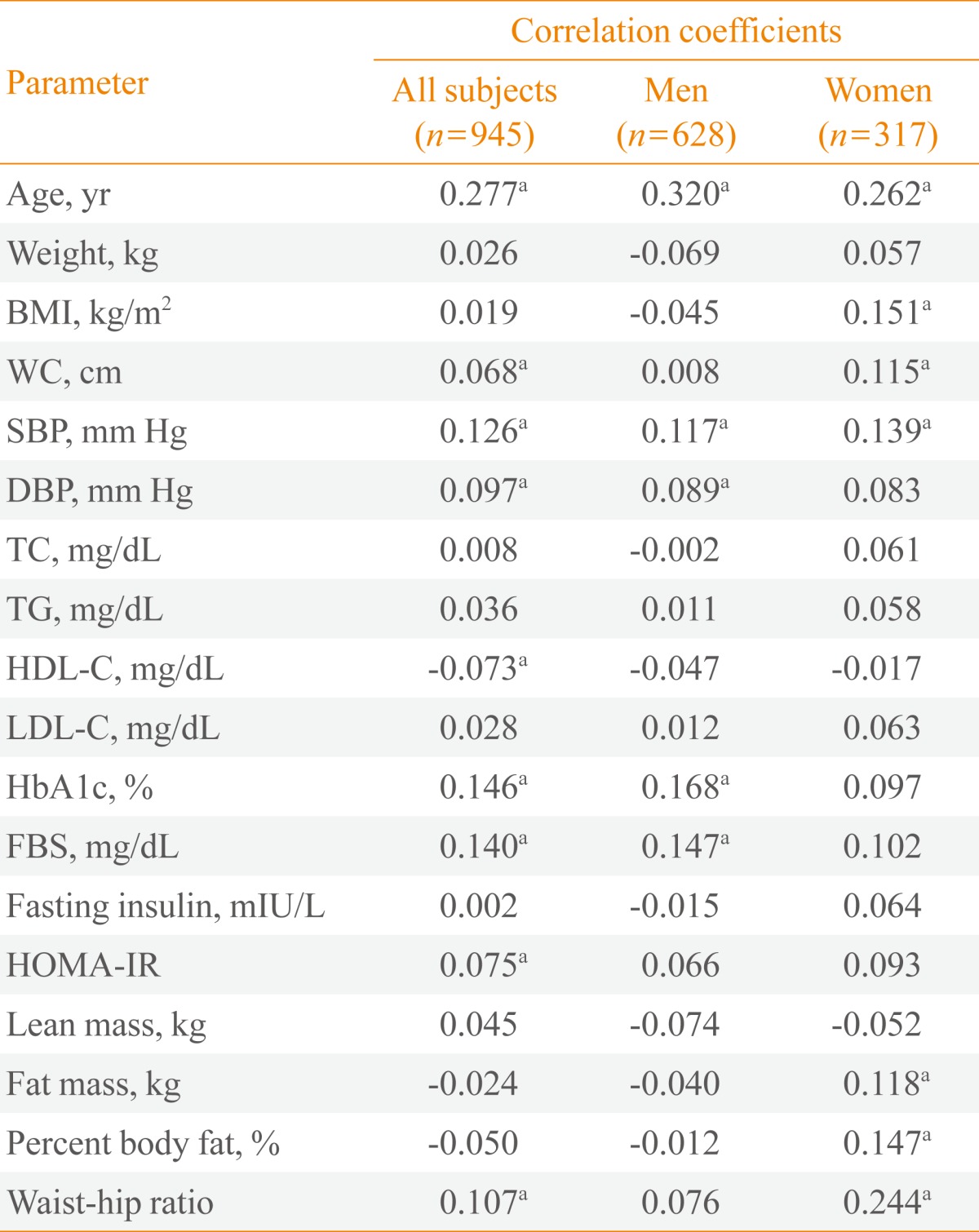
BMI, body mass index; WC, waist circumference; SBP, systolic blood pressure; DBP, diastolic blood pressure; TC, total cholesterol; TG, triglyceride; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; HbA1c, hemoglobin A1c; FBS, fasting blood sugar; HOMA-IR, homeostasis model assessment of insulin resistance.
aP<0.05 in bivariate correlation analyses with Pearson's correlation analyses.
Values are expressed as mean±standard deviation.
CACS, coronary artery calcification score; BMI, body mass index; WC, waist circumference; SBP, systolic blood pressure; DBP, diastolic blood pressure; TC, total cholesterol; TG, triglyceride; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; HbA1c, hemoglobin A1c; HOMA-IR, homeostasis model assessment of insulin resistance.
aP values for the comparison of the mean values among the three groups divided according to the CACS analyzed by one-way analysis of variance test; b,c,dSame or different letters denote significant or no differences between the designated groups in post-hoc analysis. If not designated, they are the opposite of the designated groups.
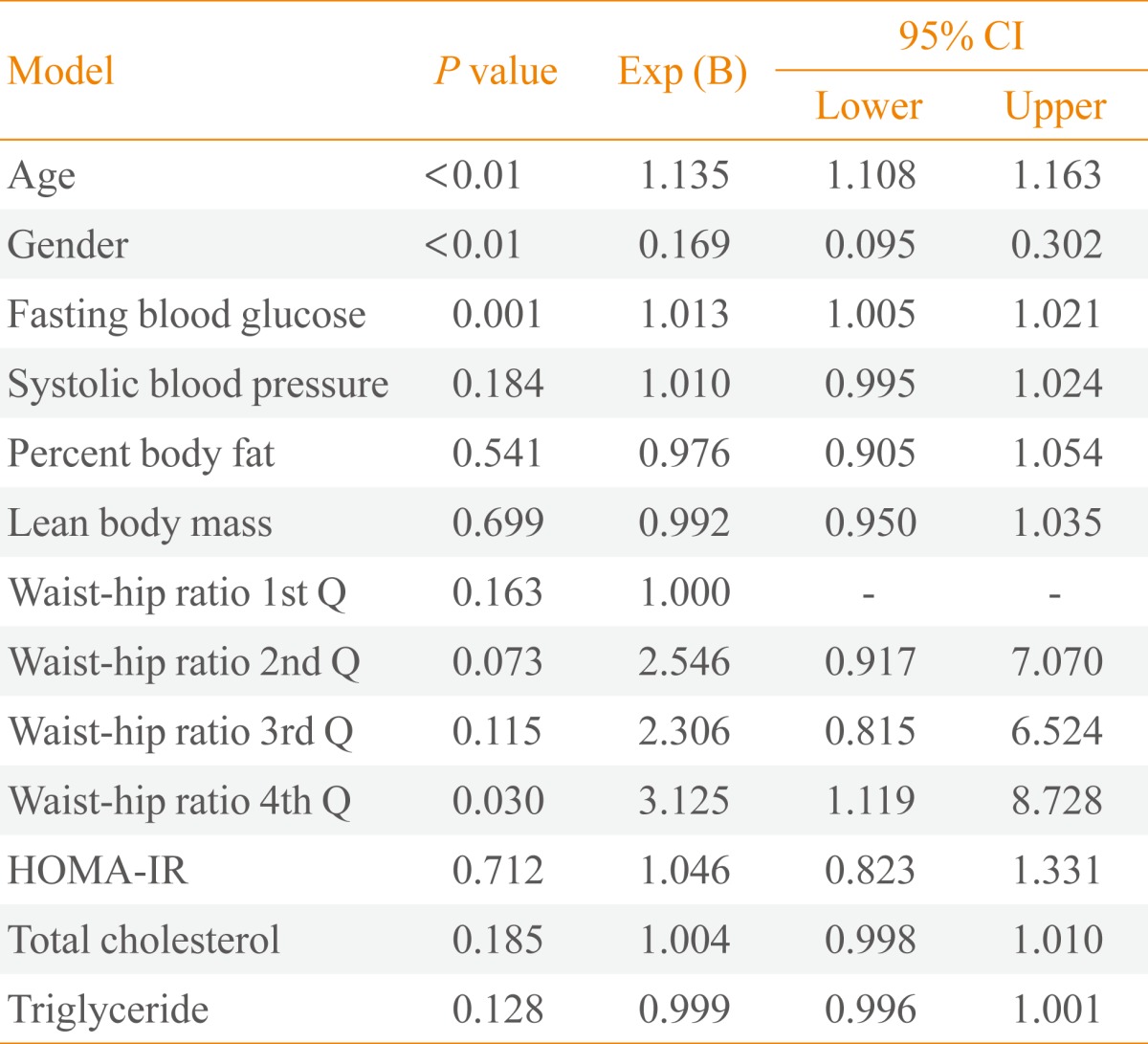
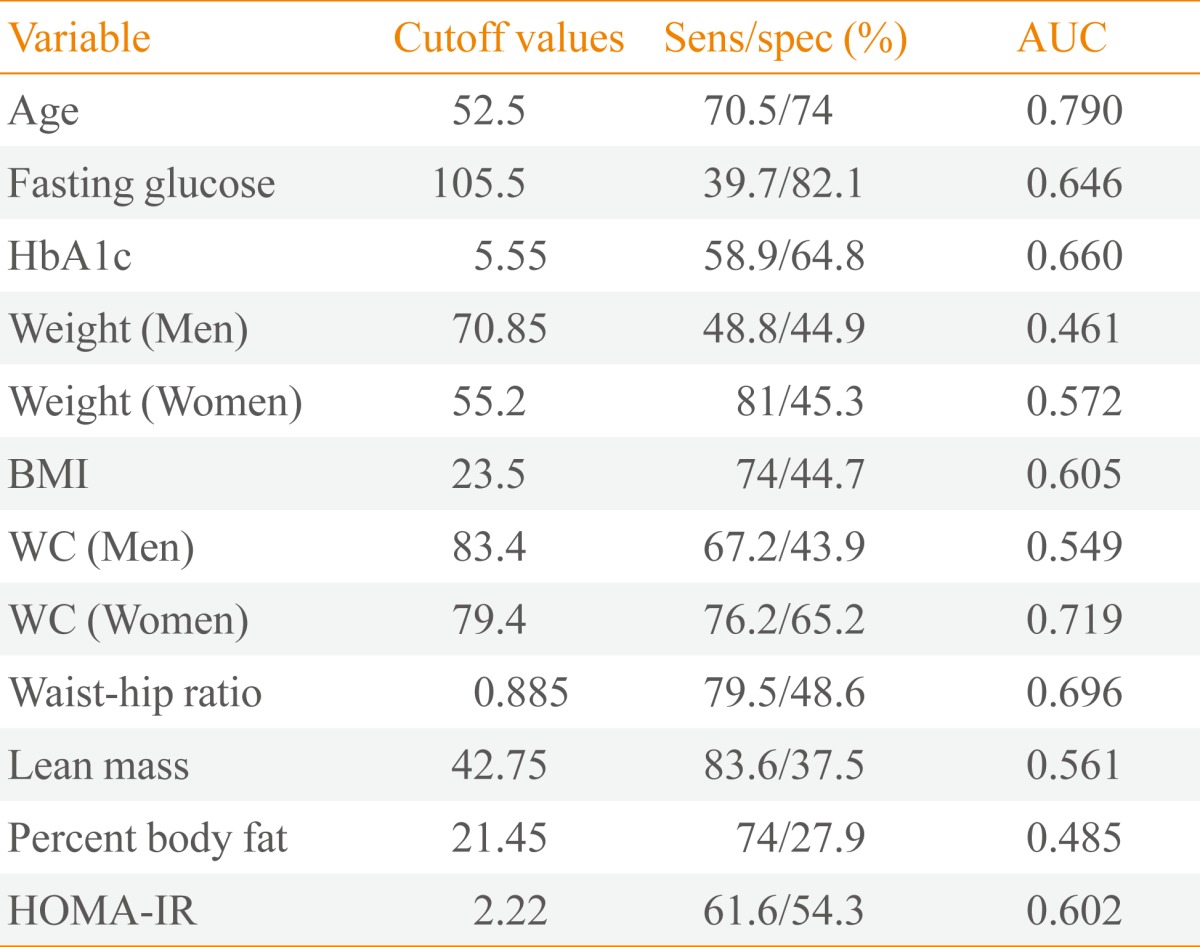
Figure & Data
References
Citations
- Body weight at age 20 and in midlife is more important than weight gain for coronary atherosclerosis: Results from SCAPIS
Göran Bergström, Annika Rosengren, Elin Bacsovics Brolin, John Brandberg, Kerstin Cederlund, Gunnar Engström, Jan E. Engvall, Maria J. Eriksson, Isabel Gonçalves, Emil Hagström, Stefan K. James, Tomas Jernberg, Mikael Lilja, Martin Magnusson, Anders Perss
Atherosclerosis.2023; 373: 46. CrossRef - Association Between Measures of Body Composition and Coronary Calcium: Findings From the Multi‐Ethnic Study of Atherosclerosis
Tamara Horwich, Preethi Srikanthan, Anisha Gaitonde, Karol Watson, Matthew Allison, Richard Kronmal
Journal of the American Heart Association.2023;[Epub] CrossRef - Pericardial fat, thoracic peri-aortic adipose tissue, and systemic inflammatory marker in nonalcoholic fatty liver and abdominal obesity phenotype
Chun-Ho Yun, Jing-Rong Jhuang, Meng-Ting Tsou
Scientific Reports.2022;[Epub] CrossRef - Gender-Based Association of Coronary Artery Calcification and Framingham Risk Score With Non-alcoholic Fatty Liver Disease and Abdominal Obesity in Taiwanese Adults, a Cross-Sectional Study
Meng-Ting Tsou, Jau-Yuan Chen
Frontiers in Cardiovascular Medicine.2022;[Epub] CrossRef - New Model for Predicting the Presence of Coronary Artery Calcification
Samel Park, Min Hong, HwaMin Lee, Nam-jun Cho, Eun-Young Lee, Won-Young Lee, Eun-Jung Rhee, Hyo-Wook Gil
Journal of Clinical Medicine.2021; 10(3): 457. CrossRef - Association between waist-hip ratio and coronary artery calcification in postmenopausal women
Youngmi Eun, Su Nam Lee, Jin Jung, Min Sik Kim, Keon-Woong Moon, Ki-Dong Yoo
Menopause.2020; 27(9): 1010. CrossRef - Being Metabolically Healthy, the Most Responsible Factor for Vascular Health
Eun-Jung Rhee
Diabetes & Metabolism Journal.2018; 42(1): 19. CrossRef - Moderate Beer Intake and Cardiovascular Health in Overweight Individuals
Teresa Padro, Natàlia Muñoz-García, Gemma Vilahur, Patricia Chagas, Alba Deyà, Rosa Antonijoan, Lina Badimon
Nutrients.2018; 10(9): 1237. CrossRef - Effects of Low-density Lipoprotein Cholesterol on Coronary Artery Calcification Progression According to High-density Lipoprotein Cholesterol Levels
Da Young Lee, Ji Hyun Kim, Se Eun Park, Cheol-young Park, Ki-won Oh, Sung-woo Park, Eun-Jung Rhee, Won-young Lee
Archives of Medical Research.2017; 48(3): 284. CrossRef - Decreased muscle mass in Korean subjects with intracranial arterial stenosis: The Kangbuk Samsung Health Study
Ho-Jung Jung, Hwanseok Jung, Taeyoung Lee, Jongho Kim, Jongsin Park, Hacsoo Kim, Junghwan Cho, Won-Young Lee, Sung-Woo Park, Eun-Jung Rhee, Hyung-Geun Oh
Atherosclerosis.2017; 256: 89. CrossRef - Analysis and comparison of statin prescription patterns and outcomes according to clinical department
H.-S. Kim, H. Kim, H. Lee, B. Park, S. Park, S.-H. Lee, J. H. Cho, H. Song, J. H. Kim, K.-H. Yoon, I. Y. Choi
Journal of Clinical Pharmacy and Therapeutics.2016; 41(1): 70. CrossRef - Increased risk for development of coronary artery calcification in insulin-resistant subjects who developed diabetes: 4-year longitudinal study
Eun-Jung Rhee, Ji Hyun Kim, Hye-Jeong Park, Se Eun Park, Hyung-Geun Oh, Cheol-Young Park, Won-Young Lee, Ki-Won Oh, Sung-Woo Park
Atherosclerosis.2016; 245: 132. CrossRef - Waist Circumference as a Marker of Obesity Is More Predictive of Coronary Artery Calcification than Body Mass Index in Apparently Healthy Korean Adults: The Kangbuk Samsung Health Study
Jongsin Park, Eun Seo Lee, Da Young Lee, Jihyun Kim, Se Eun Park, Cheol-Young Park, Won-Young Lee, Ki-Won Oh, Sung-Woo Park, Eun-Jung Rhee
Endocrinology and Metabolism.2016; 31(4): 559. CrossRef - Increased Risk of Progression of Coronary Artery Calcification in Male Subjects with High Baseline Waist-to-Height Ratio: The Kangbuk Samsung Health Study
Hyung-Geun Oh, Shriram Nallamshetty, Eun-Jung Rhee
Diabetes & Metabolism Journal.2016; 40(1): 54. CrossRef - Characteristics of Body Composition and Muscle Strength of North Korean Refugees during South Korean Stay
Sun Wook Cho, So Hee Lee, Eun Sil Koh, Si Eun Kim, Seok Joong Kim
Endocrinology and Metabolism.2015; 30(4): 551. CrossRef - Higher association of coronary artery calcification with non-alcoholic fatty liver disease than with abdominal obesity in middle-aged Korean men: the Kangbuk Samsung Health Study
Min-Kyung Lee, Hye-Jeong Park, Won Seon Jeon, Se Eun Park, Cheol-Young Park, Won-Young Lee, Ki-Won Oh, Sung-Woo Park, Eun-Jung Rhee
Cardiovascular Diabetology.2015;[Epub] CrossRef - Increased Risk for Intracranial Arterial Stenosis in Subjects With Coronary Artery Calcification
Hyung-Geun Oh, Pil-Wook Chung, Eun-Jung Rhee
Stroke.2015; 46(1): 151. CrossRef - Metabolic syndrome criteria as predictors of subclinical atherosclerosis based on the coronary calcium score
Mi Hae Seo, Eun-Jung Rhee, Se Eun Park, Cheol Young Park, Ki Won Oh, Sung Woo Park, Won-Young Lee
The Korean Journal of Internal Medicine.2015; 30(1): 73. CrossRef - Statin eligibility and cardiovascular risk burden assessed by coronary artery calcium score: Comparing the two guidelines in a large Korean cohort
Eun-Jung Rhee, Se Eun Park, Hyung Geun Oh, Cheol-Young Park, Ki-Won Oh, Sung-Woo Park, Ron Blankstein, Jorge Plutzky, Won-Young Lee
Atherosclerosis.2015; 240(1): 242. CrossRef - Relationship of Glycated Hemoglobin A1c, Coronary Artery Calcification and Insulin Resistance in Males Without Diabetes
Chan-Hee Jung, Eun-Jung Rhee, Kyu-Jin Kim, Bo-Yeon Kim, Se Eun Park, Yoosoo Chang, Seungho Ryu, Cheol-Young Park, Ji-Oh Mok, Ki-Won Oh, Chul-Hee Kim, Sung-Woo Park, Sung-Koo Kang, Won-Young Lee
Archives of Medical Research.2015; 46(1): 71. CrossRef - Metabolic Health Is a More Important Determinant for Diabetes Development than Simple Obesity: A 4-Year Retrospective Longitudinal Study
Eun-Jung Rhee, Min Kyung Lee, Jong Dae Kim, Won Seon Jeon, Ji Cheol Bae, Se Eun Park, Cheol-Young Park, Ki-Won Oh, Sung-Woo Park, Won-Young Lee, Reury F. P. Bacurau
PLoS ONE.2014; 9(5): e98369. CrossRef - Brief Review of Articles in 'Endocrinology and Metabolism' in 2013
Won-Young Lee
Endocrinology and Metabolism.2014; 29(3): 251. CrossRef - Letter: The Relationship of Body Composition and Coronary Artery Calcification in Apparently Healthy Korean Adults (Endocrinol Metab 2013;28:33-40, Jung-Hee Yu et al.)
Han Seok Choi
Endocrinology and Metabolism.2013; 28(2): 153. CrossRef - Metabolic Health Is More Closely Associated with Coronary Artery Calcification than Obesity
Eun-Jung Rhee, Mi Hae Seo, Jong Dae Kim, Won Seon Jeon, Se Eun Park, Cheol-Young Park, Ki-Won Oh, Sung-Woo Park, Won-Young Lee, Rozemarijn Vliegenthart
PLoS ONE.2013; 8(9): e74564. CrossRef
 PubReader
PubReader Cite
Cite


