Articles
- Page Path
- HOME > Endocrinol Metab > Volume 29(3); 2014 > Article
-
Original ArticleClinical Study Testosterone Deficiency Associated with Poor Glycemic Control in Korean Male Diabetics
- Joo-Sung Kim, Bong Sun Kim, Ja Young Jeon, Yong Jun Choi, Yoon-Sok Chung
-
Endocrinology and Metabolism 2014;29(3):300-306.
DOI: https://doi.org/10.3803/EnM.2014.29.3.300
Published online: September 25, 2014
Department of Endocrinology and Metabolism, Ajou University School of Medicine, Suwon, Korea.
- Corresponding author: Yoon-Sok Chung. Department of Endocrinology and Metabolism, Ajou University School of Medicine, 206 World cup-ro, Yeongtong-gu, Suwon 443-721, Korea. Tel: +82-31-219-5127, Fax: +82-31-219-4497, yschung@ajou.ac.kr
Copyright © 2014 Korean Endocrine Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- Recent studies have shown that men with diabetes have lower testosterone levels than healthy men. However, studies on the correlation between testosterone and diabetes are rare in Korea. We examined the relationship between testosterone deficiency and markers related to diabetes in adult Korean men.
-
Methods
- A total 464 men with diabetes who visited an outpatient clinic at Ajou University Hospital and had serum total testosterone and serum insulin levels measured between January 2000 and September 2013 were selected. Blood samples were collected after the subjects had fasted overnight. We divided the participants into testosterone deficient and normal groups. Testosterone deficiency was defined as having a serum total testosterone level <3.5 ng/mL.
-
Results
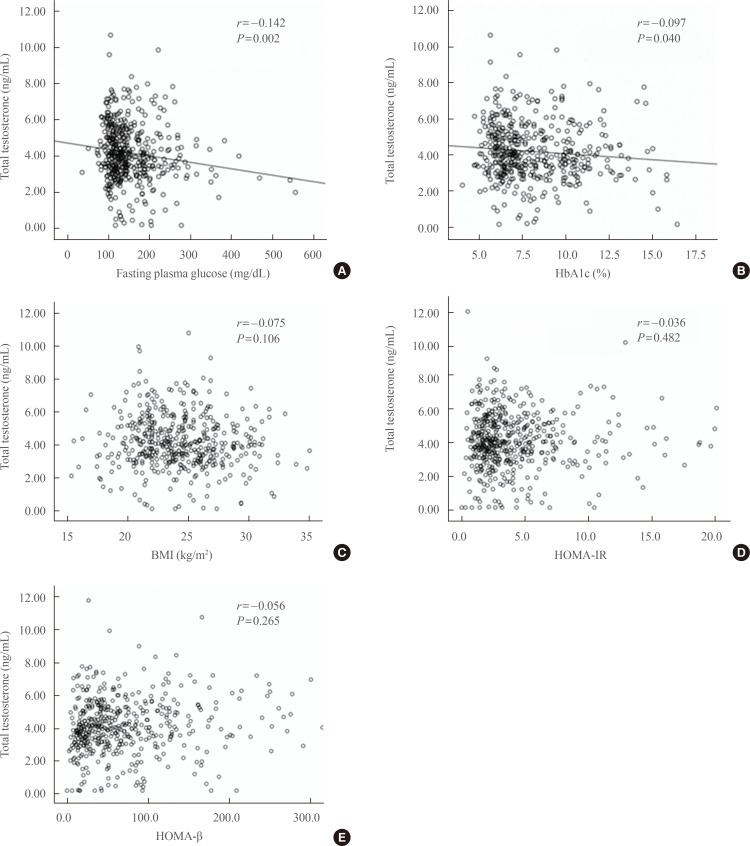
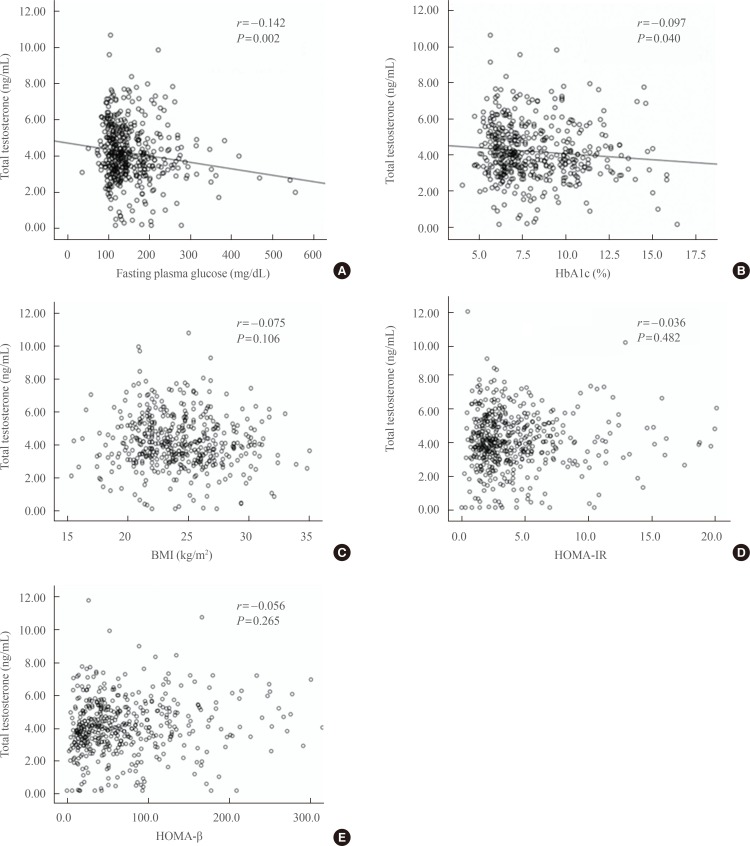
- Of 464 subjects, 34.9% had a testosterone deficiency. The mean levels of fasting plasma glucose (P=0.007) and glycated hemoglobin (HbA1c; P=0.038) were significantly higher in the testosterone deficiency group than in the normal group. To clarify the relationship between serum total testosterone level and fasting plasma glucose or HbA1c values, Pearson's correlation test was performed. Fasting plasma glucose levels (r=-0.142, P=0.002) and HbA1c values (r=-0.097, P=0.040) showed a significant negative correlation with serum testosterone levels in men with diabetes.
-
Conclusion
- Major markers of diabetes that are associated with testosterone deficiency are fasting plasma glucose and HbA1c values. Poor glycemic control appears to be associated with testosterone deficiency in Korean men with diabetes.
- Cross-sectional epidemiologic studies have reported a relationship between male hypogonadism and diabetes [1,2]. A recent analysis of 1,292 men from Norfolk, England, found that low endogenous testosterone and sex hormone binding globulin levels are associated with glycemia, even below the threshold for diabetes in middle-aged and older men [1]. In a meta-analysis that included 28 cross-sectional studies, total testosterone was lower in men with diabetes compared with controls, and diabetes remained associated with lower total testosterone levels independent of age and body mass index (BMI) [2].
- The role of insulin resistance could be one of the most important explanations of the relationship between male hypogonadism and diabetes. Previous studies have shown that hypogonadism is associated with upper abdominal adiposity and insulin resistance [3,4]. Treating systemic insulin resistance with rosiglitazone leads to only a modest increase in testosterone concentrations in men with type 2 diabetes [5], despite the restoration of normal testosterone concentrations. Moreover, results from the Massachusetts Male Aging Study suggest that low testosterone concentrations might play a role in the development of insulin resistance and subsequent type 2 diabetes [6].
- Although some studies that have replaced testosterone found no effect on glycemic control in hypogonadal subjects with type 2 diabetes [7,8], many recent studies suggest that administration of testosterone improves insulin sensitivity and glucose homeostasis in subjects with type 2 diabetes and hypogonadism [9,10,11]. With these studies, it can be speculated that endogenous testosterone levels might influence glycemic control in subjects with type 2 diabetes. However, there are only a few studies on the relationship between endogenous testosterone levels and markers related to glycemic control in Korea [12,13].
- Hence, we examined the prevalence of testosterone deficiency in subjects with type 2 diabetes and assessed the relationship between testosterone deficiency and markers related to diabetes to understand the association between testosterone and glycemic control in a Korean, diabetic population.
INTRODUCTION
- Materials
- A cross-sectional study was conducted among 464 diabetic men aged 20 years or older attending the outpatient clinic at Ajou University Hospital who had serum total testosterone and serum insulin levels measured between January 2000 and September 2013. We examined the subjects through a chart review and excluded those who had a pituitary or testicular disease, or were using testosterone, antiandrogen treatment, antifungal drugs, or steroidal agents that could affect serum testosterone levels.
- Measurements
- Height and body weight were measured by standard methods. BMI was calculated as weight divided by height squared (kg/m2). Blood pressure was measured after a period of 30 minutes rest. Blood samples were collected after the subjects had fasted overnight. Venous blood samples were collected for measuring serum total testosterone, fasting plasma glucose, glycated hemoglobin (HbA1c), serum insulin, connecting peptide (C-peptide), total cholesterol, triglyceride, high density lipoprotein cholesterol, blood urea nitrogen, and serum creatinine values. The homeostatic model assessment-insulin resistance (HOMA-IR) was calculated as fasting insulin concentration (µIU/L)×fasting glucose concentration (mg/dL)/405 [14]. The homeostatic model assessment of β-cell function (HOMA-β) was calculated as 360×fasting insulin concentration (µIU/L)/(fasting glucose concentration (mg/dL)-63) [14]. Total testosterone was measured by radioimmunoassay (Coat-A-Count, Siemens Healthcare Diagnostics, Los Angeles, CA, USA). The intra-assay coefficient of variation (CV) was 5%, for total testosterone concentrations of 4.00 ng/mL. The interassay CV was 6.7%, for total testosterone concentrations of 4.01 ng/mL.
- Statistical analysis
- Testosterone deficiency was defined as having a serum total testosterone level <3.5 ng/mL [15,16,17]. Continuous variables were expressed as mean±SD, and categorical variables were expressed as numbers (n) and percentage (%). The t test was performed for continuous variables to compare the testosterone deficiency group and the normal testosterone group. Pearson's correlation coefficients were calculated to evaluate the relationship between serum total testosterone levels and variables (fasting plasma glucose, HbA1c, BMI, HOMA-IR, and HOMA-β). Data processing and statistical analyses were performed using SPSS version 18.0 (IBM Co., Armonk, NY, USA). P<0.05 were considered statistically significant.
METHODS
- The baseline characteristics of the subjects are shown in Table 1. The mean age of the participants was 52.3 years (range, 20 to 85), and mean BMI, systolic blood pressure (SBP), and diastolic blood pressure (DBP) were 24.2 kg/m2, 125.1, and 76.1 mm Hg, respectively. The mean duration of diabetes was 40.4 months. Mean levels of fasting plasma glucose, HbA1c, serum insulin, and C-peptide were 8.1%, 156.0 mg/dL, 15.7 µIU/mL, and 3.0 ng/mL, respectively. The mean level of total testosterone was 4.2 ng/mL.
- In all, 34.9% of men had testosterone deficiency (162/464). The subjects were divided into two groups: a testosterone deficient group (total testosterone <3.5 ng/mL) and a normal group (total testosterone ≥3.5 ng/mL). The t test was performed to identify significantly different parameters between the two groups. We found that age, BMI, SBP, DBP, and the duration of diabetes were not significantly different between the two groups (P=0.397, P=0.912, P=0.924, P=0.968, and P=0.133). However, the parameters related to glycemic control-fasting plasma glucose and HbA1c-were significantly different between the two groups. Mean fasting plasma glucose levels in the testosterone deficient and normal groups were 165.0 and 146.6 mg/dL, respectively (P=0.007). The mean HbA1c levels in the testosterone deficient and normal groups were 8.4% and 8.0%, respectively (P=0.038). No significant differences were observed in other parameters between the testosterone deficient and normal groups (Table 2).
- Subsequently, Pearson's correlation coefficients were calculated to evaluate the relationship between fasting plasma glucose, HbA1c, BMI, HOMA-IR, HOMA-β, and serum total testosterone values. As shown in Fig. 1, Pearson's coefficient correlation (r) between total testosterone and fasting plasma glucose levels was -0.142 and the P value was 0.002. The estimated regression relation was: testosterone=4.743-0.004×fasting plasma glucose (Fig. 1A). Thus, testosterone decreased 0.004 ng/mL with a 1 mg/dL increase in fasting plasma glucose. Pearson's coefficient correlation (r) between total testosterone and HbA1c levels was -0.097 and the P value was 0.040. The estimated regression relation was: testosterone=4.782-0.067×HbA1c (Fig. 1B). Thus, testosterone decreased 0.067 ng/mL as HbA1c levels increased 1%. However, BMI, HOMA-IR, and HOMA-β were not statistically correlated with serum total testosterone levels (P=0.106, P=0.482, and P=0.265) (Fig. 1C-E).
RESULTS
- In this study, the prevalence of testosterone deficiency in diabetic men was 34.9%. The testosterone deficiency group showed significantly higher fasting plasma glucose and HbA1c levels compared to the normal group. Serum total testosterone levels were negatively correlated with fasting plasma glucose and HbA1c levels in Korean, diabetic men.
- In previous studies, serum testosterone levels were shown to be negatively correlated with fasting plasma glucose levels, HbA1c values, and insulin sensitivity [4,18,19]. However, the debate continues. Corrales et al. [20] demonstrated that total testosterone levels are positively correlated with HbA1c levels, but not correlated with fasting plasma glucose, insulin, or C-peptide levels. Therefore, the relationship between total testosterone levels and markers of diabetes (fasting plasma glucose, HbA1c, serum insulin, C-peptide, HOMA-IR, and HOMA-β values) was evaluated in Korean, diabetic subjects.
- In this study, fasting plasma glucose and HbA1c levels were significantly higher in the testosterone deficient group than in the normal group. However, we could not find any significant differences in parameters related to insulin resistance and insulin secretion. C-peptide and serum insulin levels are indicators of insulin secretion. HOMA-IR, which is a marker of insulin resistance, and HOMA-β, which is a marker of β-cell function, were calculated using fasting insulin levels. Therefore, testosterone levels might be associated with glycemic control, but are not associated with insulin resistance or insulin secretion.
- Previous studies have demonstrated that insulin resistance is associated with low serum testosterone levels in men because testosterone affects insulin sensitivity by controlling the glycogen synthesis system, particularly in muscle [21,22,23]. Moreover, Heufelder et al. [24] suggested the beneficial effects of testosterone administration on insulin resistance in patients with diabetes. However in our study, no significant relationship was found between serum total testosterone and serum insulin, serum C-peptide, HOMA-IR, or HOMA-β values, which are directly related with serum insulin levels.
- As an explanation for this discrepancy, it could be suggested that glycemic control might modulate testosterone levels. In another study, improved glycemic control using rosiglitazone increased testosterone levels in subjects with diabetes [5]. In addition, several studies evaluated the association of hypogonadotropic hypogonadism and diabetes [25,26,27,28]. George et al. [29] demonstrated that the pathophysiology of hypogonadism in men with type 2 diabetes is related to a hypothalamic neuropeptide named kisspeptin, which is down-regulated with hyperglycemia in animal studies [30]. In that study, kisspeptin administration increased luteinizing hormone (LH) pulse frequency and LH secretion, as a result enhancing endogenous testosterone secretion in hypotestosteronaemic men with type 2 diabetes.
- The present study has several limitations. First, this study was cross sectional and a single hospital-based study. Thus, the results cannot be generalized to all patients with diabetes. Second, performing a single laboratory measurement of serum testosterone is a pitfall for making an erroneous diagnosis of testosterone deficiency; it has been reported that about 30% of such men may have normal testosterone levels on repeat measurements [31]. Third, we did not assess free testosterone and bioavailable testosterone. Some investigators have suggested that testosterone deficiency in patients with lower total testosterone levels should be confirmed by testing levels of free testosterone, which might correlate better with the biological activities of androgen than total testosterone. Fourth, we examined the duration of diabetes of the participants, but not a medication history of diabetes, which could affect glycemic control.
- In conclusion, the prevalence of testosterone deficiency in men with diabetes was 34.9% in our study. Among markers related to diabetes, fasting plasma glucose and HbA1c levels-and not serum insulin, C-peptide, HOMA-IR, and HOMA-β-were associated with testosterone deficiency. Our findings suggest that poor glycemic control is associated with testosterone deficiency in Korean, male diabetics.
DISCUSSION
- 1. Brand JS, Wareham NJ, Dowsett M, Folkerd E, van der Schouw YT, Luben RN, Khaw KT. Associations of endogenous testosterone and SHBG with glycated haemoglobin in middle-aged and older men. Clin Endocrinol (Oxf) 2011;74:572–578. ArticlePubMed
- 2. Corona G, Monami M, Rastrelli G, Aversa A, Sforza A, Lenzi A, Forti G, Mannucci E, Maggi M. Type 2 diabetes mellitus and testosterone: a meta-analysis study. Int J Androl 2011;34(6 Pt 1):528–540. ArticlePubMed
- 3. Haffner SM. Sex hormones, obesity, fat distribution, type 2 diabetes and insulin resistance: epidemiological and clinical correlation. Int J Obes Relat Metab Disord 2000;24(Suppl 2):S56–S58. ArticlePubMedPDF
- 4. Laaksonen DE, Niskanen L, Punnonen K, Nyyssonen K, Tuomainen TP, Salonen R, Rauramaa R, Salonen JT. Sex hormones, inflammation and the metabolic syndrome: a population-based study. Eur J Endocrinol 2003;149:601–608. ArticlePubMed
- 5. Kapoor D, Channer KS, Jones TH. Rosiglitazone increases bioactive testosterone and reduces waist circumference in hypogonadal men with type 2 diabetes. Diab Vasc Dis Res 2008;5:135–137. ArticlePubMed
- 6. Stellato RK, Feldman HA, Hamdy O, Horton ES, McKinlay JB. Testosterone, sex hormone-binding globulin, and the development of type 2 diabetes in middle-aged men: prospective results from the Massachusetts male aging study. Diabetes Care 2000;23:490–494. ArticlePubMed
- 7. Lee CH, Kuo SW, Hung YJ, Hsieh CH, He CT, Yang TC, Lian WC, Chyi-Fan S, Pei D. The effect of testosterone supplement on insulin sensitivity, glucose effectiveness, and acute insulin response after glucose load in male type 2 diabetics. Endocr Res 2005;31:139–148. ArticlePubMed
- 8. Basu R, Dalla Man C, Campioni M, Basu A, Nair KS, Jensen MD, Khosla S, Klee G, Toffolo G, Cobelli C, Rizza RA. Effect of 2 years of testosterone replacement on insulin secretion, insulin action, glucose effectiveness, hepatic insulin clearance, and postprandial glucose turnover in elderly men. Diabetes Care 2007;30:1972–1978. ArticlePubMed
- 9. Kapoor D, Goodwin E, Channer KS, Jones TH. Testosterone replacement therapy improves insulin resistance, glycaemic control, visceral adiposity and hypercholesterolaemia in hypogonadal men with type 2 diabetes. Eur J Endocrinol 2006;154:899–906. ArticlePubMed
- 10. Marin P, Holmang S, Jonsson L, Sjostrom L, Kvist H, Holm G, Lindstedt G, Bjorntorp P. The effects of testosterone treatment on body composition and metabolism in middle-aged obese men. Int J Obes Relat Metab Disord 1992;16:991–997. PubMed
- 11. Boyanov MA, Boneva Z, Christov VG. Testosterone supplementation in men with type 2 diabetes, visceral obesity and partial androgen deficiency. Aging Male 2003;6:1–7. ArticlePubMed
- 12. Han H, Shin JH, Lee CB, Park YS, Kim DS, Ahn YH, Kim TW, Choi WH. The relation of the testosterone level with metabolic syndrome and coronary artery disease in Korean middle-aged and elderly men. Korean J Med 2007;73:34–43.
- 13. Kim S, Rhee EJ, Seok HS, Choi YG, Chung WG, Lee DY, Kim SY, Jung CH, Park CY, Lee WY, Oh KW, Park SW, Kim SW. The association of sex hormones and the metabolic syndrome in apparently healthy Korean male adults. Korean J Med 2007;73:565–574.
- 14. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985;28:412–419. ArticlePubMedPDF
- 15. Page ST, Amory JK, Bowman FD, Anawalt BD, Matsumoto AM, Bremner WJ, Tenover JL. Exogenous testosterone (T) alone or with finasteride increases physical performance, grip strength, and lean body mass in older men with low serum T. J Clin Endocrinol Metab 2005;90:1502–1510. ArticlePubMed
- 16. Hildreth KL, Barry DW, Moreau KL, Vande Griend J, Meacham RB, Nakamura T, Wolfe P, Kohrt WM, Ruscin JM, Kittelson J, Cress ME, Ballard R, Schwartz RS. Effects of testosterone and progressive resistance exercise in healthy, highly functioning older men with low-normal testosterone levels. J Clin Endocrinol Metab 2013;98:1891–1900. ArticlePubMedPMCPDF
- 17. Basaria S, Coviello AD, Travison TG, Storer TW, Farwell WR, Jette AM, Eder R, Tennstedt S, Ulloor J, Zhang A, Choong K, Lakshman KM, Mazer NA, Miciek R, Krasnoff J, Elmi A, Knapp PE, Brooks B, Appleman E, Aggarwal S, Bhasin G, Hede-Brierley L, Bhatia A, Collins L, LeBrasseur N, Fiore LD, Bhasin S. Adverse events associated with testosterone administration. N Engl J Med 2010;363:109–122. ArticlePubMedPMC
- 18. Fukui M, Soh J, Tanaka M, Kitagawa Y, Hasegawa G, Yoshikawa T, Miki T, Nakamura N. Low serum testosterone concentration in middle-aged men with type 2 diabetes. Endocr J 2007;54:871–877. ArticlePubMed
- 19. Pitteloud N, Mootha VK, Dwyer AA, Hardin M, Lee H, Eriksson KF, Tripathy D, Yialamas M, Groop L, Elahi D, Hayes FJ. Relationship between testosterone levels, insulin sensitivity, and mitochondrial function in men. Diabetes Care 2005;28:1636–1642. ArticlePubMed
- 20. Corrales JJ, Burgo RM, Garca-Berrocal B, Almeida M, Alberca I, Gonzalez-Buitrago JM, Orfao A, Miralles JM. Partial androgen deficiency in aging type 2 diabetic men and its relationship to glycemic control. Metabolism 2004;53:666–672. ArticlePubMed
- 21. Holmang A, Svedberg J, Jennische E, Bjorntorp P. Effects of testosterone on muscle insulin sensitivity and morphology in female rats. Am J Physiol 1990;259(4 Pt 1):E555–E560. ArticlePubMed
- 22. Holmang A, Larsson BM, Brzezinska Z, Bjorntorp P. Effects of short-term testosterone exposure on insulin sensitivity of muscles in female rats. Am J Physiol 1992;262(6 Pt 1):E851–E855. ArticlePubMed
- 23. Holmang A, Bjorntorp P. The effects of cortisol on insulin sensitivity in muscle. Acta Physiol Scand 1992;144:425–431. ArticlePubMed
- 24. Heufelder AE, Saad F, Bunck MC, Gooren L. Fifty-two-week treatment with diet and exercise plus transdermal testosterone reverses the metabolic syndrome and improves glycemic control in men with newly diagnosed type 2 diabetes and subnormal plasma testosterone. J Androl 2009;30:726–733. ArticlePubMed
- 25. Kapoor D, Aldred H, Clark S, Channer KS, Jones TH. Clinical and biochemical assessment of hypogonadism in men with type 2 diabetes: correlations with bioavailable testosterone and visceral adiposity. Diabetes Care 2007;30:911–917. ArticlePubMed
- 26. Rhoden EL, Ribeiro EP, Teloken C, Souto CA. Diabetes mellitus is associated with subnormal serum levels of free testosterone in men. BJU Int 2005;96:867–870. ArticlePubMed
- 27. Grossmann M, Thomas MC, Panagiotopoulos S, Sharpe K, Macisaac RJ, Clarke S, Zajac JD, Jerums G. Low testosterone levels are common and associated with insulin resistance in men with diabetes. J Clin Endocrinol Metab 2008;93:1834–1840. ArticlePubMedPDF
- 28. Corona G, Mannucci E, Petrone L, Ricca V, Balercia G, Mansani R, Chiarini V, Giommi R, Forti G, Maggi M. Association of hypogonadism and type II diabetes in men attending an outpatient erectile dysfunction clinic. Int J Impot Res 2006;18:190–197. ArticlePubMedPDF
- 29. George JT, Veldhuis JD, Tena-Sempere M, Millar RP, Anderson RA. Exploring the pathophysiology of hypogonadism in men with type 2 diabetes: kisspeptin-10 stimulates serum testosterone and LH secretion in men with type 2 diabetes and mild biochemical hypogonadism. Clin Endocrinol (Oxf) 2013;79:100–104. ArticlePubMed
- 30. Castellano JM, Navarro VM, Fernandez-Fernandez R, Roa J, Vigo E, Pineda R, Dieguez C, Aguilar E, Pinilla L, Tena-Sempere M. Expression of hypothalamic KiSS-1 system and rescue of defective gonadotropic responses by kisspeptin in streptozotocin-induced diabetic male rats. Diabetes 2006;55:2602–2610. ArticlePubMed
- 31. Brambilla DJ, O'Donnell AB, Matsumoto AM, McKinlay JB. Intraindividual variation in levels of serum testosterone and other reproductive and adrenal hormones in men. Clin Endocrinol (Oxf) 2007;67:853–862. ArticlePubMed
References
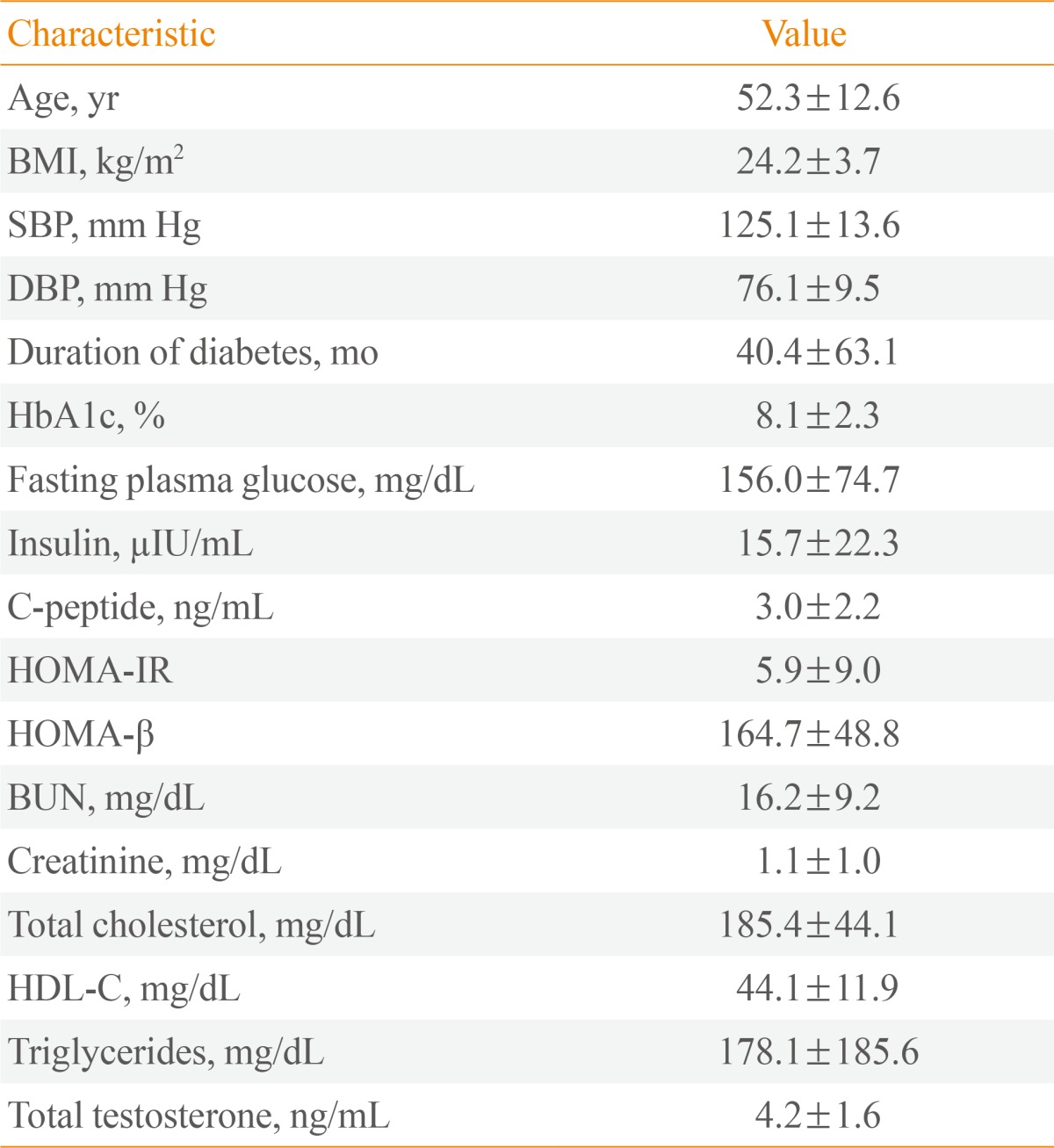
Values are expressed as mean±SD.
BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; HbA1c, glycated hemoglobin; C-peptide, connecting peptide; HOMA-IR, homeostatic model assessment-insulin resistance; HOMA-β, homeostatic model assessment-β cell function; BUN, blood urea nitrogen; HDL-C, high density lipoprotein cholesterol.
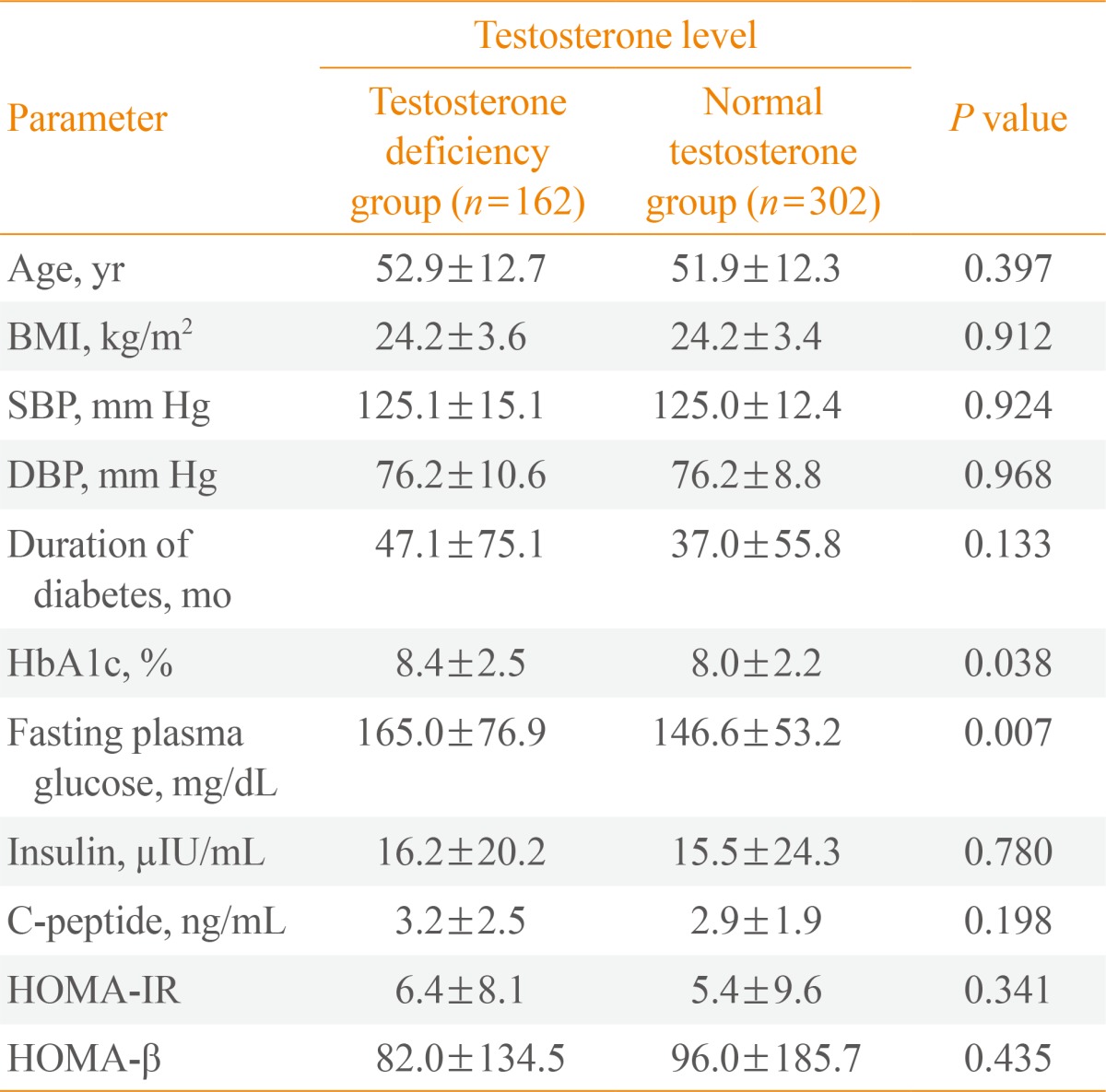
Figure & Data
References
Citations
- Association between T2DM and the lowering of testosterone levels among Kashmiri males
Rabia Farooq, Mohammad Hayat Bhat, Sabhiya Majid, Mohammad Muzaffar Mir
Archives of Endocrinology and Metabolism.2020;[Epub] CrossRef - Hypogonadism and associated risk factors in male patients with type 2 diabetes mellitus attending the diabetic clinic of Tikur Anbessa Specialized Teaching Hospital, Addis Ababa, Ethiopia
Sisay Teka, Samuel Kinde, Gobena Dedefo, Kissi Mudi, Getahun Tarekegn
Journal of Endocrinology, Metabolism and Diabetes of South Africa.2019; 24(1): 16. CrossRef - Hypogonadism in Nigerian men with type 2 diabetes mellitus
S. I. Onung, E. E. Young, T. E. Ugwu, O. A. Fasanmade
International Journal of Diabetes in Developing Countries.2017; 37(3): 254. CrossRef - Articles in 'Endocrinology and Metabolism' in 2014
Won-Young Lee
Endocrinology and Metabolism.2015; 30(1): 47. CrossRef
 PubReader
PubReader Cite
Cite